
It is common to see patients who tell us: “Doctor, when I smile I have a tooth that is misplaced. It’s a dark spot: we only see that, I don’t dare to smile anymore! “. They tell us regarding a tooth in the incisor-canine sector in the palatal or lingual position. This break in alignment creates an unsightly gray area in the smile which tends to increase with a loss of occlusal stability. The tooth, which is more difficult to brush and therefore poorly cleaned, is also prone to plaque retention. What solution can we offer our patients? A dental veneer?
Orthodontics, dental veneer
If the tooth is healthy and intact, the solution of choice is orthodontics to restore the position on the dental arch and occlusal stability.
« To achieve the aesthetic goals of tooth position and angulation, many patients with aesthetic problems require orthodontic treatment. (Riedel 1950; Peck and Peck 1970). But the constraints associated with this technique put off some of our adult patients.
A discolored tooth or one whose physical integrity is altered (enamel fracture, caries, etc.) will ultimately require a aesthetic restoration.
Advantages and disadvantages…
compared
Orthodontics
Advantages
Respect for the integrity of the dental organ.
Alignment of arches.
Disadvantages
Duration of treatment.
Discomfort (gutters).
Unsightly (rings).
Contention indispensable.
No treatment of dyschromias or anatomical defects.
Dental veneer
« For malformed, misplaced, or slightly damaged teeth, direct and indirect bonded dental materials can restore esthetics and create a pleasing smile with minimal invasion and limited sacrifice of natural tooth structure. » (Bayne et al. 2019).
Advantages
Quick treatment (1 or 2 appointments depending on the technique).
No contention.
Associated treatment of dischromies and anatomical defects.
Inconvenience
Requires touching the integrity of the dental tissue (enamel).
CAD/CAM technique
For equipped practices, CAD/CAM (computer-aided design and manufacturing) makes it possible to prepare, design and place the prosthetic element in the same session. Recent studies attest to a good success rate for this technique (87.5% up to 27 years (Otto 2017), 93.5% following 10 years (Beier et al. 2012).
Advantages
Time saving for the patient (1 single trip).
Avoids the installation and removal of a temporary.
Inconvenience
Requires a good mastery of the technique for a satisfactory aesthetic result.
Clinical case – dental veneer
Sabra, 30, presents with 31 in the lingual position. The patient tells us that the position of her tooth is changing and is more and more linguo-versed (Fig.1, 2). We offer him, as first intention, a treatment with alignment gutters in order to reposition the incisor (31) on the arch. Our patient refuses, given the constraints and the duration of the orthodontic treatment, but asks us for another therapeutic alternative.

Fig.1, 2: Dent 31 linguo-versée.
Dental veneer made in the office by CAD/CAM
1 – Preparation
A preparation a minima of the recipient dental organ preserves the tissues and the vitality of the tooth. It is essential to preserve the enamel to ensure effective bonding. Less is more. The minimum thickness of the ceramic veneer (Vita Mk2) is 0.3 mm + the bonding (NX3) 0.1 mm. Occlusal coverage 0.5 mm. The tooth in the lingual position is just “frosted” vestibular. A positioning groove is created around the edge of the bonding of the future veneer with a diamond bur calibrated at 0.1 mm (Fig.3). The occlusal edge is reduced by 0.5 mm.

Fig.3: Preparation.
2 – Optical impression taking
In the practice, we are equipped with the “Trios 3shape intraoral scanner” camera (Fig.4 to 8).

Fig.4: Optical impression taking.

Fig.5 to 8: Optical impression (3Shape). Fig.5: Antagonist.

Fig.6: Mandibular arch.
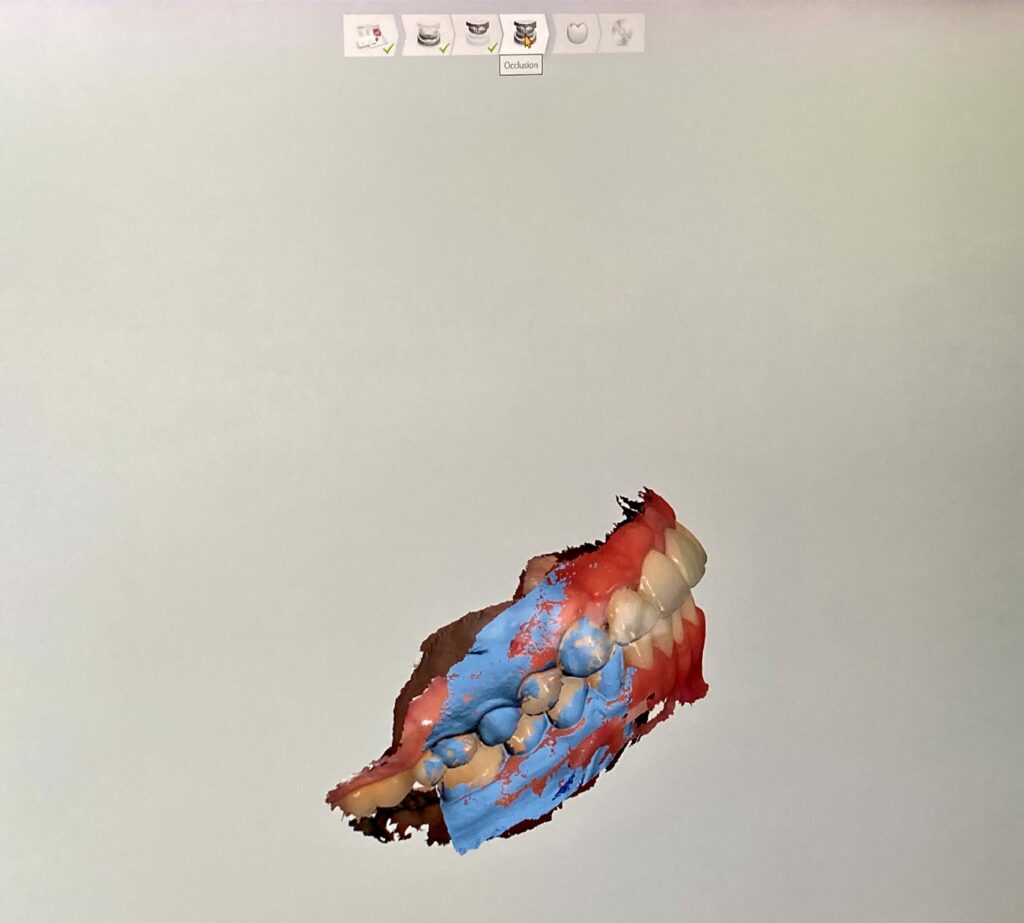
Fig.7, 8 : Occlusion.

3 – Modeling
The digital impression is saved as an STL file and imported into our modeling software “Inlab” (Sirona) (Fig.9 to 14).
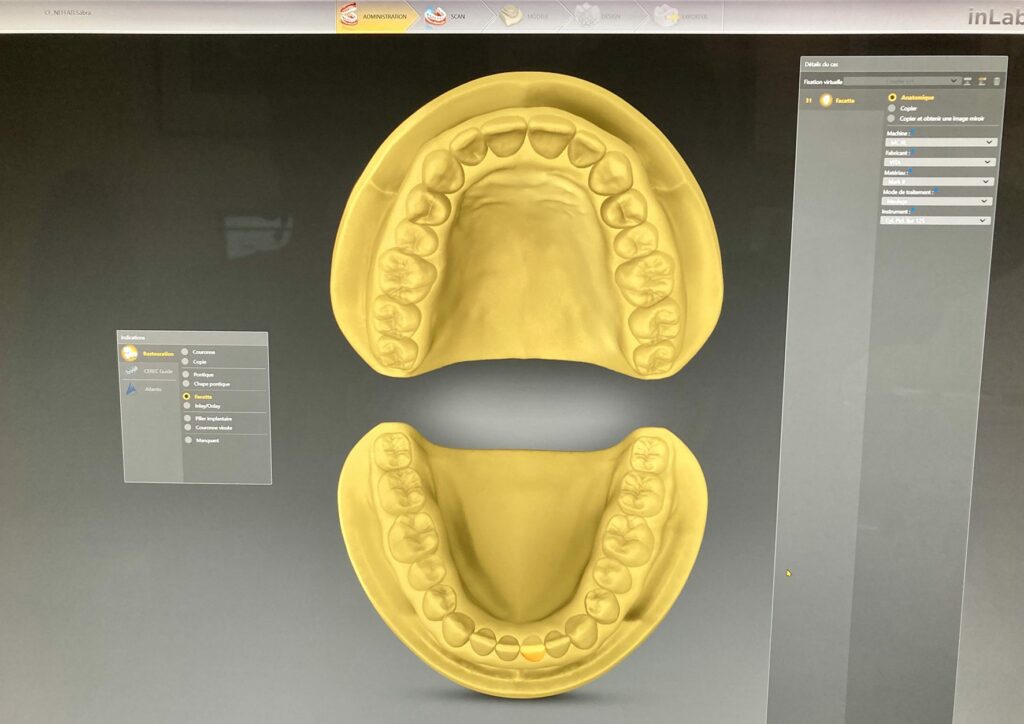
Fig.9: Inlab software opening page.
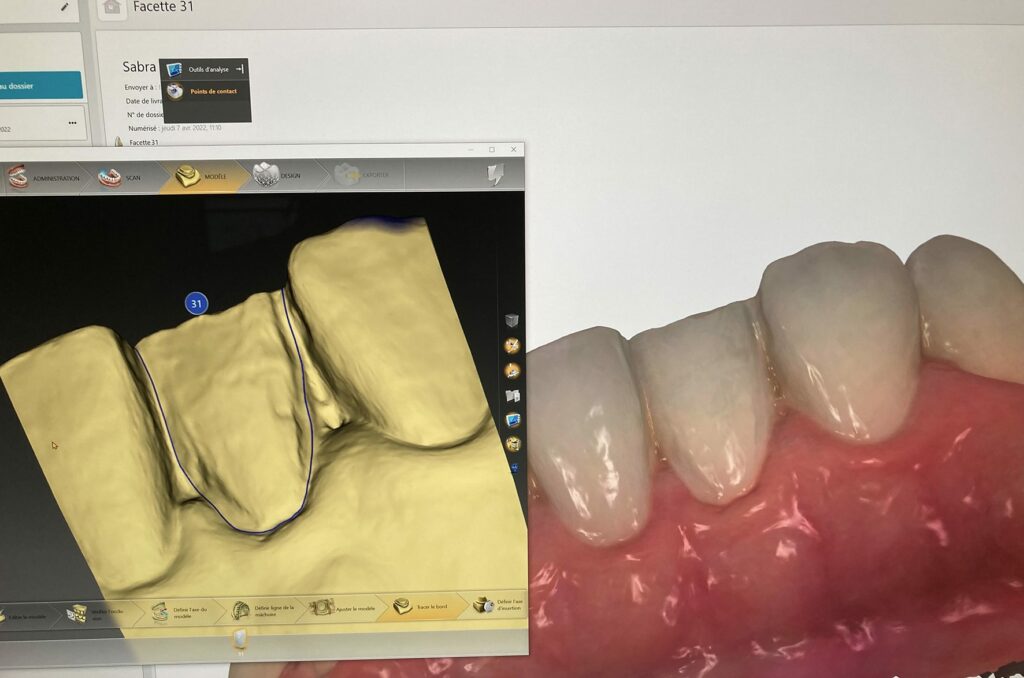
Fig.10: 3Shape and Inlab software superimposed.

Fig.11 to 14: Design of the veneer in the “Inlab” software.
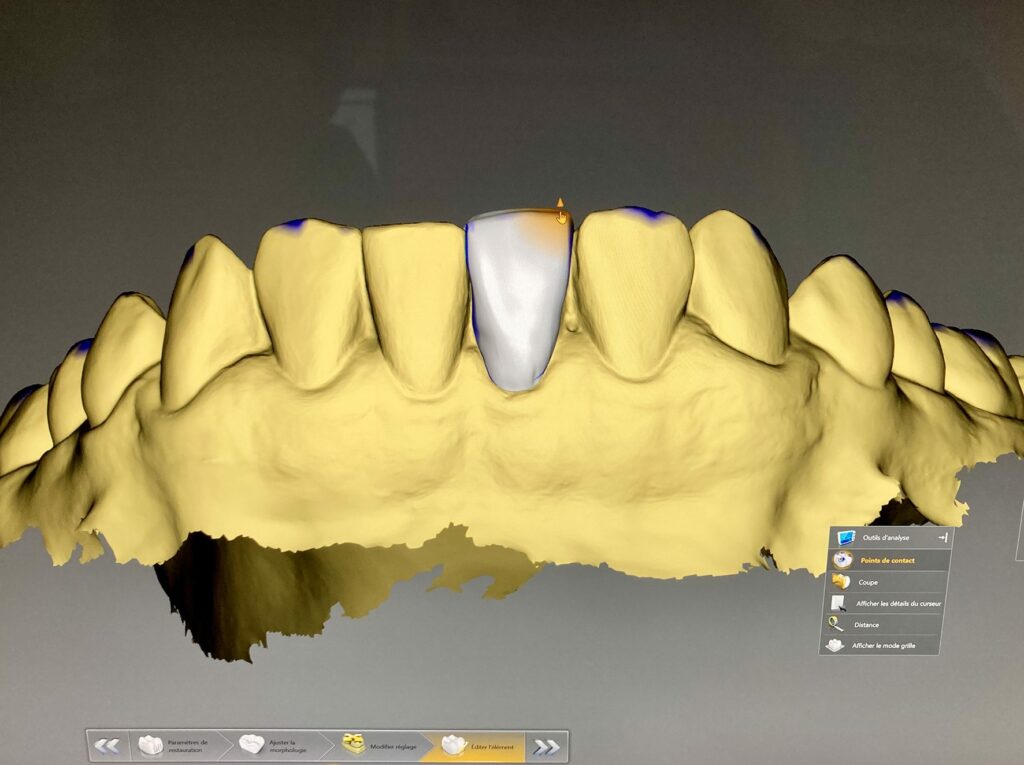
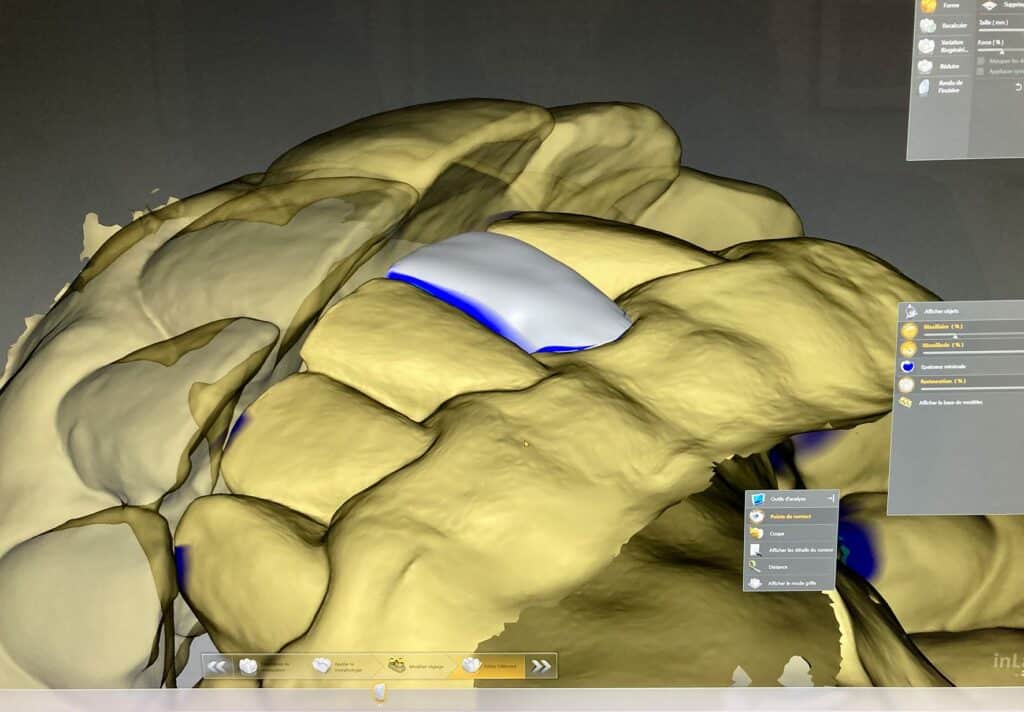
Fig.13.
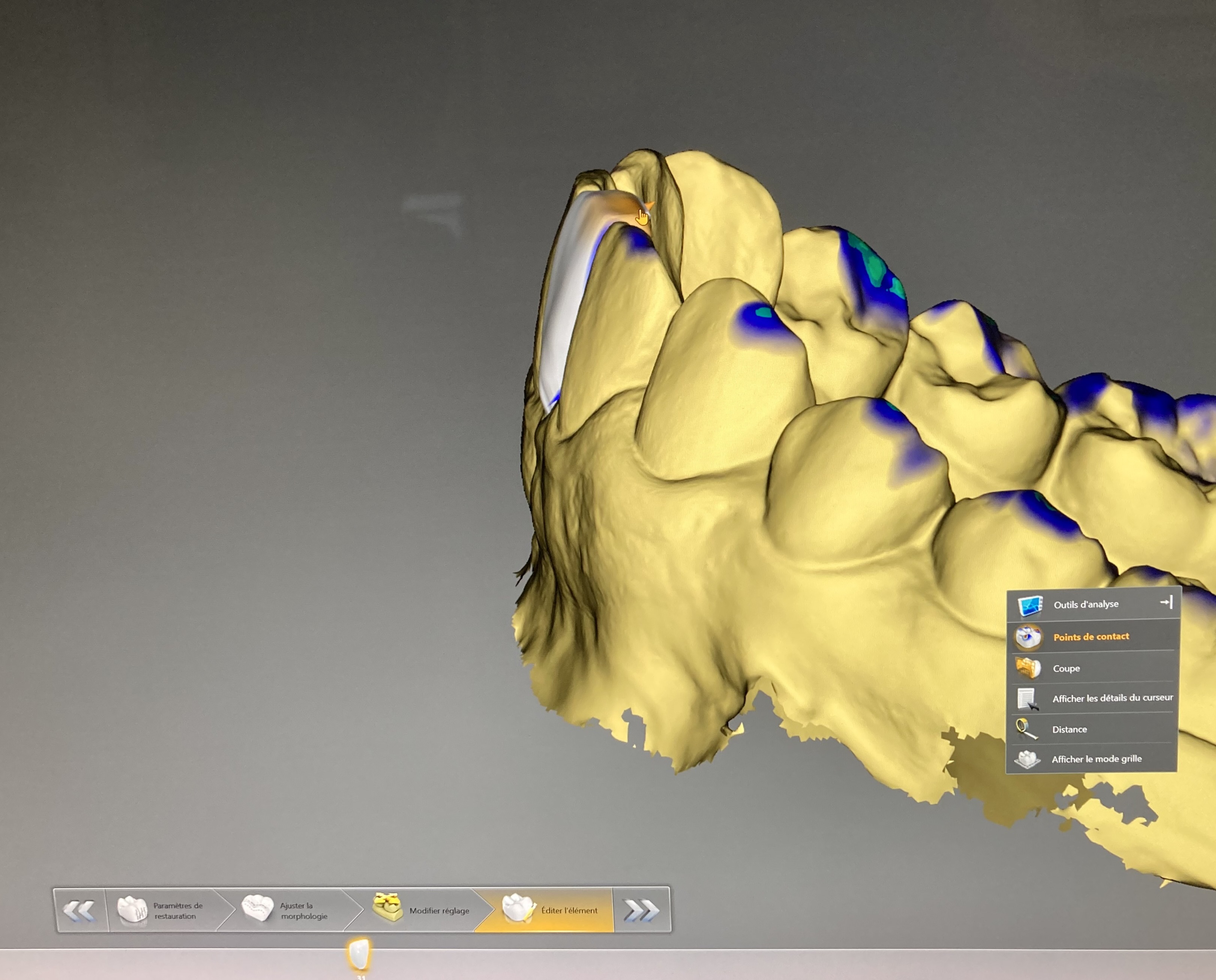
Fig.14.
4 – Machining
The virtual modeling is machined using the Inlab Cam software (Fig.15) which controls our MCXL Premium (Sirona) milling machine (Fig.17).
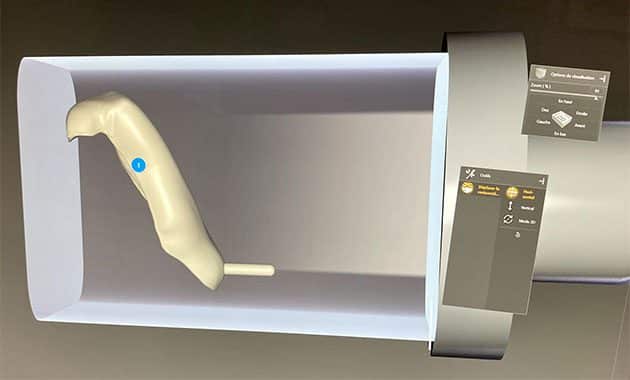

Fig.16: Vita MKII pedestal in feldspathic ceramic.

Fig.17 : Usineuse Inlab Premium.

Fig.18: Ceramic dental veneer following machining.

Fig.19: Trying on the “raw” facet in the mouth.
5 – Trying on the “raw” facet coming out of the milling machine
6 – Staining and ceramic firing
The raw veneer is placed on a firing support. After having coated the vestibular surface with a glaze (Vita Akzent plus) compatible with the feldspathic ceramic used, different stains make it possible to characterize the facet in order to integrate it as well as possible within the arch of our patient (Fig.20). .
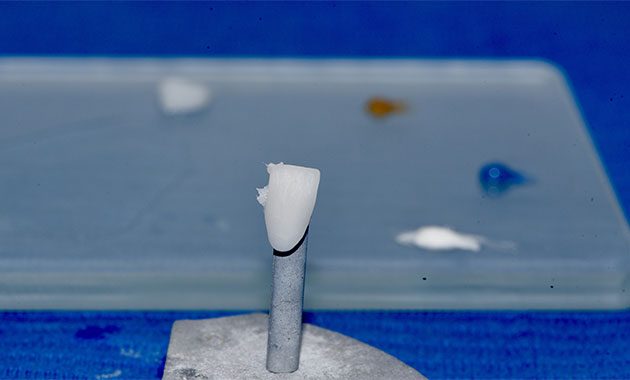
Fig.20: Facette and our make-up palette.
The ceramic oven (Vita Atmomat) is programmed to reach a firing temperature of 940° for 1 minute 30, allowing the make-up to be fixed without altering the properties of our veneer (Fig.21).

Fig.21 : Four Vita Atmomat.
7 – Collage
We have been using NX3 bonding resin (Kerr) for many years. L’intrados of the veneer is treated with 9% “Ultradent Porcelain Etch” hydrofluoric acid, rinsed and dried before applying a drop of silane. The bonding surface on the natural tooth is disinfected with chlorhexidine before treatment with a primer and an “Optibond” adhesive. NX3 Facet Bonding Resin is light-curing. A first flash with a 3-second polymerization lamp is applied, allowing easy removal of excess glue, then 40 seconds with 2 x 1200 W lamps (Fig.22 to 26).

Fig.22 : Photopolymérisation.

Fig.23: Removal of excess with dental floss.

Fig.24, 25, 26: Bonded veneer.

Fig.25.

Fig.26.
Conclusion
If orthodontic treatment remains the preferred solution for correcting a malposition, the realization of a ceramic veneer in one session (duration approximately 1 hour) can restore the harmony of the smile of our patients in a lasting way. The placement of this veneer restores the contact points with the adjacent teeth, ensuring occlusal stability. No restraint will be necessary.
Dr Cyrille FONTENEAU

Private practice in Paris
Restorative aesthetic dentistry fixed prosthesis CAD/CAM
Implant surgery
Bibliography
F.A. Spitznagel, J.Boldt, P.C. Gierthmuehlen A concept of facial esthetics.
Peck H., Peck S. Angle Orthod. 1970 CAD/CAM Ceramic Restorative Materials for Natural Teeth. Journal of Dental Research 2018.
M.B. Blatz, G. Chiche, O. Bahat, R. Roblee, C. Coachman, H.O. Heymann Evolution of Aesthetic Dentistry. Journal of Dental Research 2019.
J.R. Kelly, P. Benetti Ceramic materials in dentistry: historical evolution and current practice. Australian Dental Journal 2011.
J.J. Ten Bosch, J.C. Coop Tooth color and reflectance as related to light scattering and enamel hardness. J Dent Res 1995.
Blatz M.B., Vonderheide M., Conejo J. The Effect of Resin Bonding on Long-Term Success of High-Strength Ceramics. J Dent Res. 2018.
Arcelino Farias-Neto, Fernanda Cristina Dantas de Medeiros, Larissa Vilanova, Mariana Simonetti Chaves, Jéssica Janine Freire Batista de Araújo Tooth preparation for ceramic veneers: when less is more. int.J. Esthet. Tooth 2019
Otto T. Up to 27-years clinical long-term results of chairside Cerec 1 CAD/CAM inlays and onlays. Int J Comput Dent. 2017.
This article is for subscribers only.


