

Introduction
In this study, we aim to rigorously investigate the potential of immune checkpoint inhibitor (ICI) rechallenge to enhance survival rates among patients with extensive-stage small-cell lung cancer (ES-SCLC). Furthermore, we delve into identifying potential biomarkers that could signal which patient populations may benefit from ICI rechallenge following initial first-line treatment.
The tumor microenvironment (TME) is a critical aspect of cancer progression and has been identified as a pivotal element influencing ICI response rates. The TME is notably immunosuppressive, underlining the basis for employing ICIs in oncology. Accumulating evidence highlights that the clinical effectiveness of ICIs is intricately linked to patterns of immune cell infiltration within tumors. Therefore, we also focused our exploration on the mechanisms that contribute to the positive outcomes associated with ICI rechallenge by analyzing TME landscapes in relevant patient populations.
Methods
Study Design and Data Collection
The data utilized in this comprehensive study was sourced from the IMpower133 study (IMpower133 cohort) and from a cohort of ES-SCLC patients at Shandong Cancer Hospital and Institute (Shanzhong cohort). The IMpower133 study is a double-blind, randomized Phase I/III trial that has demonstrated that incorporating atezolizumab into a treatment regimen of carboplatin and etoposide for first-line therapy significantly improves both overall survival (OS) and progression-free survival (PFS) in comparison with a placebo combined with carboplatin and etoposide. Since the study and its accompanying data have already been published, we were not required to obtain informed consent or separate ethical committee approval. Each patient involved in this study provided written informed consent, and the study was sanctioned by the Ethics Committee of Shandong Cancer Hospital and Institute (approval ID number: 2024006145), aligning with the principles outlined in the Declaration of Helsinki. The patients recruited from both the IMpower133 study and the Shanzhong cohort underwent further analyses.
Estimation of Immune Cell Type Fractions and Gene Expressions
We downloaded the ES-SCLC bulk RNA sequencing data from IMpower133 from the European Genome-Phenome Archive. To quantify the presence of 22 immune cell types within the ES-SCLC specimens, we applied the CIBERSORT algorithm, which estimates the proportions of different cell types within a mixed cell population based on normalized data. The 22 types of immune cell infiltrates identified by CIBERSORT include B cells, plasma cells, T cells, NK cells, monocytes, macrophages, dendritic cells, mast cells, eosinophils, and neutrophils. Processed gene expression data were accessed through public databases and normalized using the limma package in R software (version 4.2.3).
Tissue Multiplex Immunofluorescent (mIF) Staining
We acquired ES-SCLC samples through biopsies, where 5 um thick formalin-fixed paraffin-embedded (FFPE) tissue sections from the Shanzhong cohort were assessed using multiplex immunofluorescence (mIF) technology. The evaluated markers included CD68 (KP1; Abcam, cat#ab955), CD206 (E6T5J; CST, cat#24595), CD4 (EPR6855; Abcam, cat#ab133616), CD45RA (D9M8I; CST, cat#13917), CCR7 (E75; Abcam, cat#ab32075), and S100A16 (Abcam, ab130419). All immunofluorescence slides received counterstaining with DAPI, and results were thoroughly reviewed by a study pathologist. Imaging scans were executed using the Vectra Polaris at 20X magnification. The patient inclusion process and overall study design are illustrated in Figure 1.
 |
Figure 1 Flow chart of included patients. A total of 201 SCLC patients from IMPower133 were assessed in the current study. After excluding patients with unknown information and those untreated after progression, we were left with 125 participants. Among these, 54 patients received atezolizumab-based treatment following initial progression, while 71 patients underwent alternative anti-cancer therapies, excluding atezolizumab, also after progression. Data collected comprised age, sex, Eastern Cooperative Oncology Group (ECOG) status, tobacco history (TOBHX), objective response rate, number of metastatic sites, body mass index (BMI), and the neutrophil to lymphocyte ratio (NLR). Furthermore, we recruited an additional 378 ES-SCLC patients receiving ICI as first-line treatment from Shandong Cancer Hospital and Institute (Shanzhong cohort). After excluding 217 patients lacking documented second-line treatment strategies, we identified a final group of 161 patients. Within this cohort, 89 patients underwent ICI retreatment while the remaining 72 received alternative treatment options. A total of 54 patients (43.20%) were exposed to atezolizumab following their first progression defined as Atezo, and 71 patients (56.80%) received non-atezolizumab therapies. The analysis of categorical variables demonstrated no significant differences in age, sex, ECOG, TOBHX, objective response, and metastatic site count between patients treated with atezolizumab and those who were not (p > 0.05 for all) (Table 1). Given that both BMI and NLR are known to influence survival within SCLC patient populations, comparisons of these continuous variables were made between the two treatment groups. |
Statistical Analysis
We utilized the χ2 test for categorical variables and the Wilcoxon rank-sum test for continuous variables to analyze differences in clinical characteristics as they pertained to atezolizumab treatment. Kaplan-Meier survival curves were plotted and subsequently compared using the log-rank test. We performed univariate and multivariate Cox regression analyses to examine the hazard ratios (HR) for overall survival among SCLC patients across various clinical factors. Additionally, the correlation between M2 macrophage infiltration and S100A16 expression was evaluated using Pearson’s χ2 test. The results of the subgroup analyses are illustrated in corresponding forest plots. All statistical computations were conducted with R software (version 4.2.3), with a p-value < 0.05 regarded as statistically significant.
Results
Clinicopathological Characteristics of ES-SCLC
A total of 201 SCLC patients from IMpower133 were included in this study. Following exclusions of individuals with missing data and untreated patients post-progression, the remaining cohort comprised 125 patients. Among these, 54 underwent atezolizumab treatment subsequent to progression, whereas 71 received other standard anti-cancer therapies, excluding atezolizumab. Comprehensive demographic data encompassed age, sex, ECOG performance status, tobacco history, objective response rates, and the count of metastatic sites. In addition, 378 ES-SCLC patients undergoing first-line ICI treatment were recruited from the Shanzhong cohort. After excluding 217 patients without established second-line treatment plans, 161 patients satisfied the inclusion criteria. Within this group, 89 patients received ICI retreatment while 72 underwent non-ICI therapies. Notably, 54 patients (43.20%) progressed to treatment with atezolizumab (Atezo) and 71 patients (56.80%) received alternative therapies. The presence of categorical baseline characteristics indicative of the recruited patient population showed no significant discrepancies in age, sex, ECOG performance status, tobacco history, and response rates based on treatment assignment to atezolizumab versus other options (p > 0.05 for all). Importantly, the median BMI in patients receiving atezolizumab was recorded at 27.95 (range: 23.50–30.30), compared to 24.97 (range: 21.85–27.72) in non-atezolizumab recipients, reflecting a statistically significant difference (p=0.016). Furthermore, patients in the cross-line treatment category who were on atezolizumab showcased a numerically lower NLR average of 2.97 (range: 2.05–5.46) against the 3.55 (range: 2.53–5.78) of non-atezolizumab counterparts.
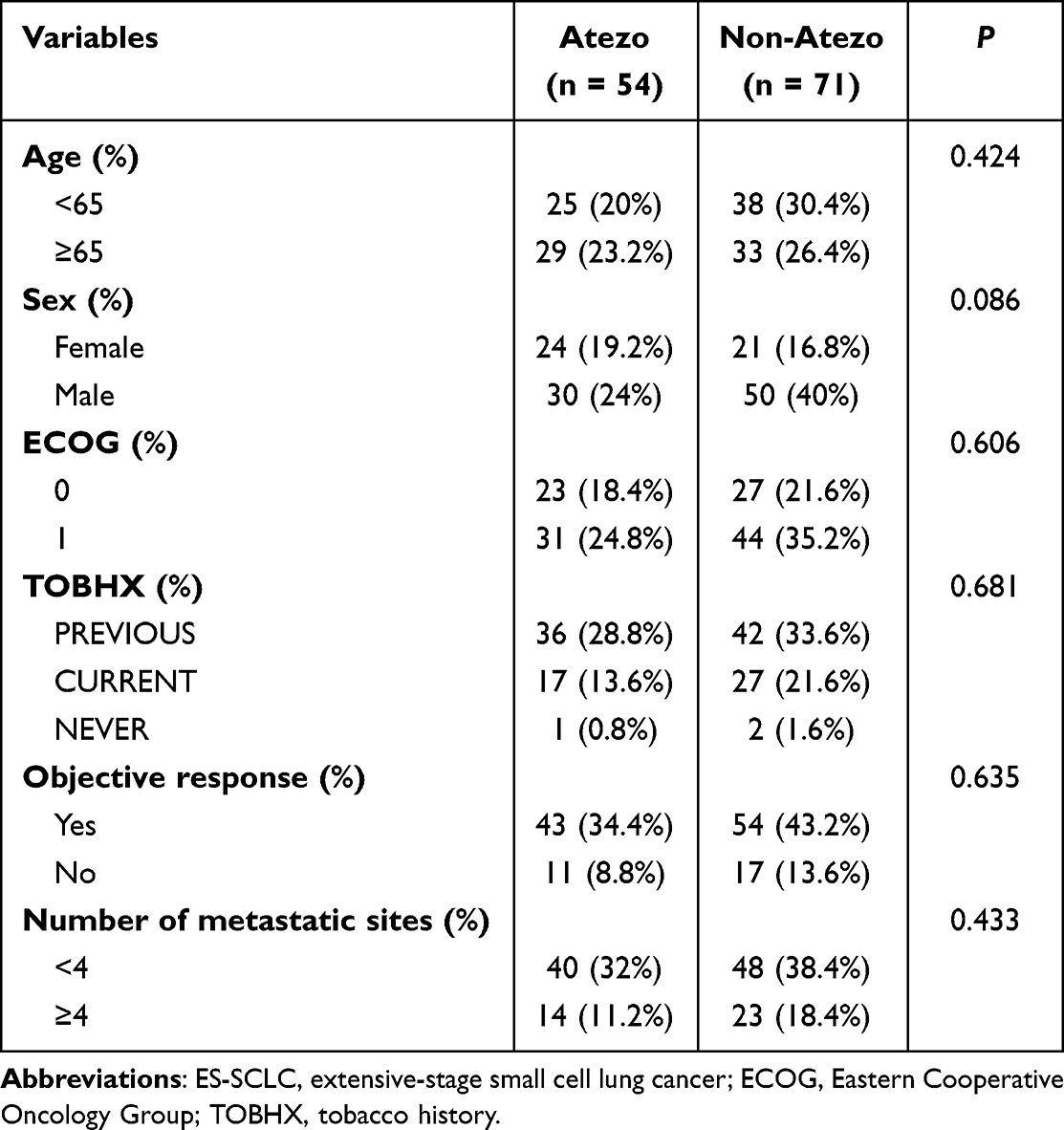 |
Table 1 Clinicopathological Characteristics of ES-SCLC
|
Survival Difference Between Atezolizumab and Non-Atezolizumab Treatment for ES-SCLC Patients Following Progression from ICI as First-Line Treatment
We evaluated the survival disparity between patients treated with atezolizumab versus those who received non-atezolizumab therapies through Kaplan-Meier analysis, focusing on ES-SCLC patients who progressed following initial ICI therapy. For these patients, those receiving atezolizumab exhibited numerically extended survival duration compared to participants without atezolizumab treatment, although this difference did not reach statistical significance (P = 0.08). Moreover, we observed that the mortality risk ratio was higher among those treated without atezolizumab following their progression. Additionally, leveraging data from the Shanzhong cohort, we established that patients receiving ICI treatment displayed significantly improved overall survival compared to non-ICI recipients following progression from first-line ICI therapy (P = 0.013). The risk of mortality remained relatively higher in non-ICI treated subjects relative to their ICI counterparts after progression.
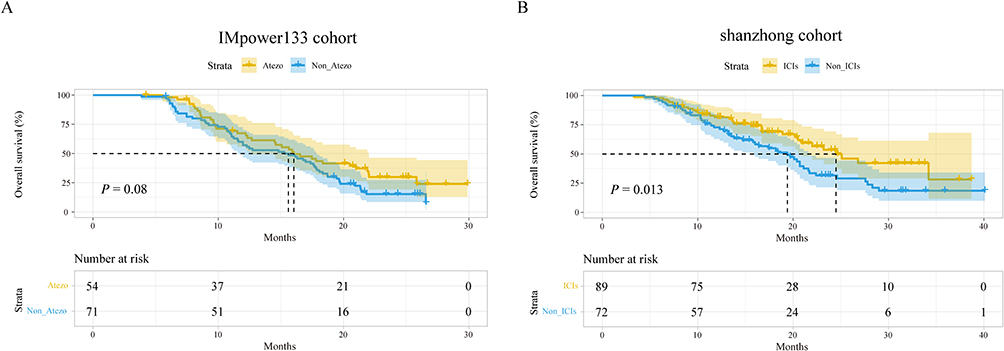 |
Figure 2 The effect of ICI rechallenge on survival among ES-SCLC patients following progression of ICI as first-line treatment. (A) Comparison of survival for ES-SCLC patients treated with atezolizumab or without atezolizumab using Kaplan Meier analysis using IMpower133 data. (B) Comparison of survival for ES-SCLC patients treated with ICI or without ICI using Kaplan Meier analysis using data from the Shanzhong cohort.
|
Beneficial Population from ICI Rechallenge
Our observations indicated a trend suggesting a numerical survival benefit for ES-SCLC patients treated with atezolizumab compared to those who received non-atezolizumab following initial line therapy. To identify critical factors that may influence survival among ES-SCLC patients who did not respond to atezolizumab as first-line treatment, we compared survival rates between groups based on multiple clinical variables, including age, sex, ECOG score, tobacco usage history, objective response, and metastatic site count. Specifically, subgroup analyses revealed a noteworthy survival benefit in patients with fewer than four metastatic sites who received atezolizumab compared to those receiving alternative therapies (HR, 0.457; 95% CI, 0.256–0.817; P = 0.008). Further validation indicated survival advantage for patients exhibiting lower numbers of metastatic sites (
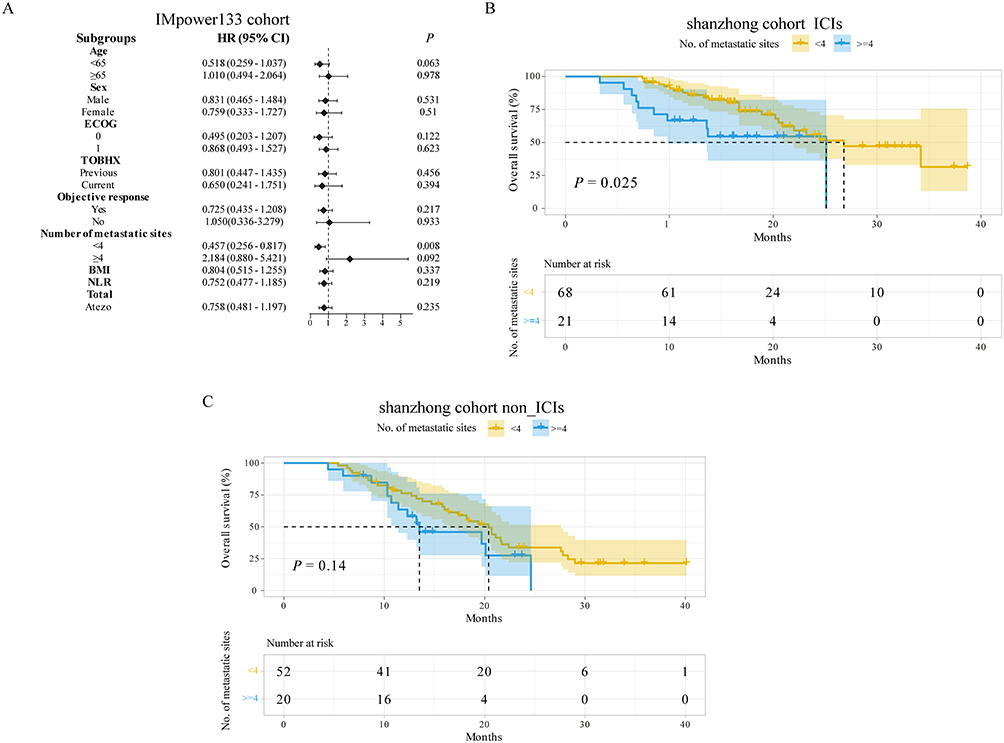 |
Figure 3 Effect of metastatic sites in affecting survival in ES-SCLC patients with and without ICI rechallenge. (A) Forest plot of subgroup analysis of survival according to clinical variables in ES-SCLC patients with atezolizumab rechallenge. Clinical variables include age, sex, ECOG, TOBHX, objective response, and number of metastatic sites. (B) The effect of metastatic sites on survival of ES-SCLC patients with ICI rechallenge. (C) The effect of metastatic sites on survival of ES-SCLC patients without ICI rechallenge.
|
ES-SCLC Patients with Metastatic Sites Less Than 4 May Derive Survival Benefit from ICI Rechallenge
Survival curves were plotted based on the overall survival from the IMpower133 cohort specifically for patients with ES-SCLC showing fewer than four metastatic sites. The results revealed that those receiving atezolizumab significantly outlived those who did not receive atezolizumab treatment (P = 0.036). This finding was corroborated using data from the Shanzhong cohort, where ES-SCLC patients harboring fewer than four metastatic sites also exhibited significantly longer overall survival in those who underwent ICI treatment than in their non-ICI counterparts following initial ICI treatment failure (P = 0.018). To validate our hypothesis regarding the survival benefit derived from ICI rechallenge in ES-SCLC patients with fewer than four metastatic sites, we employed univariate and multivariate Cox proportional hazards regression analyses to evaluate prognostic factors linked to overall survival. The multivariate Cox model analysis revealed that those treated with atezolizumab after experiencing progression (HR, 0.457; 95% CI, 0.256–0.817; P = 0.008), along with patients aged 65 years or older presenting age-related advantages (HR, 0.409; 95% CI, 0.227–0.738; P = 0.003), were recognized as protective factors yielding favorable overall survival outcomes.
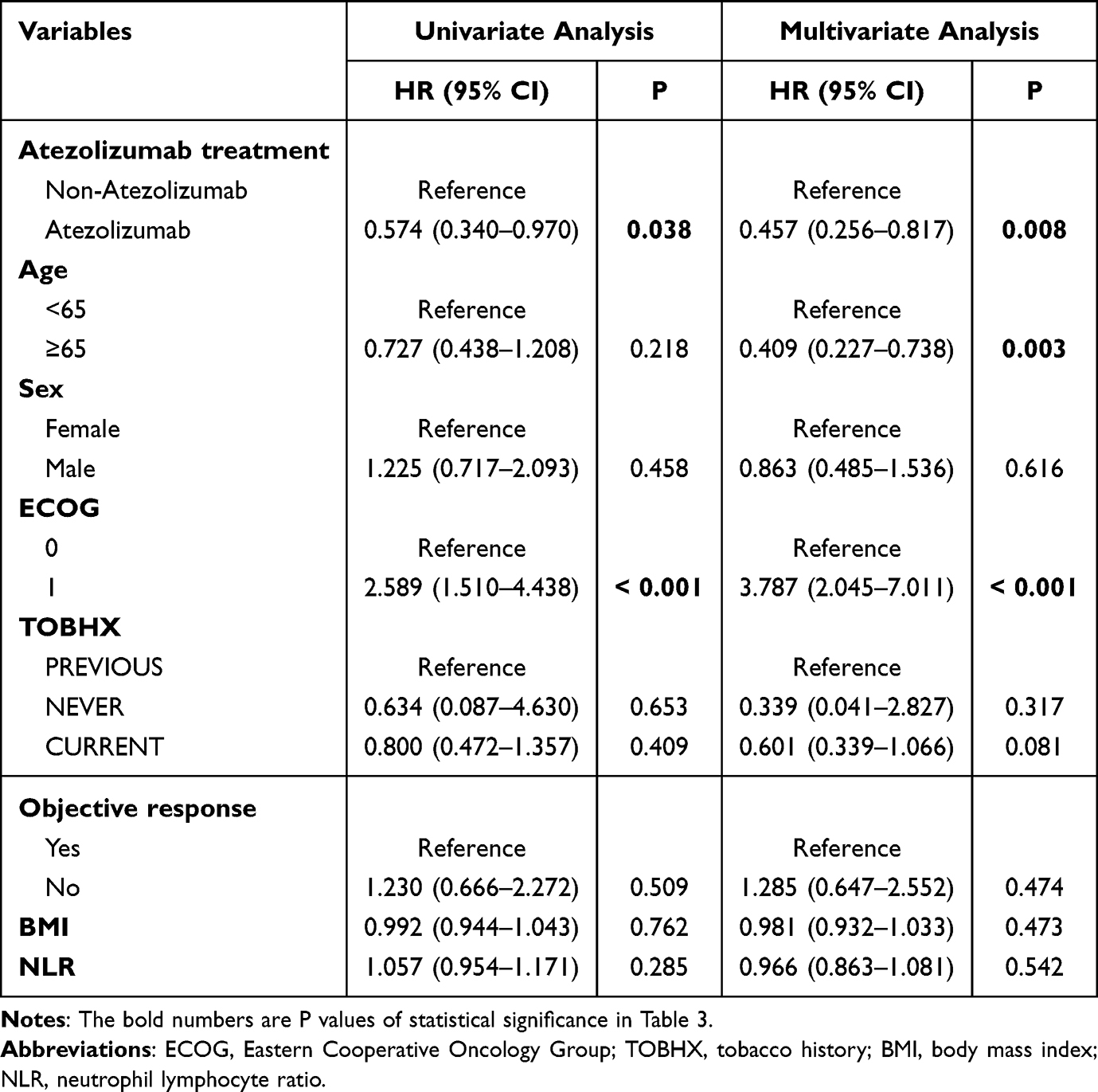 |
Table 3 The Prognostic Factors for OS Among Patients with ES-SCLC Harboring Less Than 4 Metastatic Sites Using Univariate and Multivariate Cox Proportional Hazards Regression Analyses
|
Patients with ES-SCLC Harboring Less Than 4 Metastatic Sites May Benefit from ICI Rechallenge by Reshaping Tumor Microenvironment
To investigate potential mechanisms underpinning the superior survival rates among ES-SCLC patients, we analyzed TME characteristics. Markers indicative of M2 macrophages (CD68+CD206+) and CD4 naïve T cells (CD4+CD45RA+CCR7+) within SCLC samples from the Shanzhong cohort were stained via multiplex immunofluorescence, corroborating our earlier conclusions.
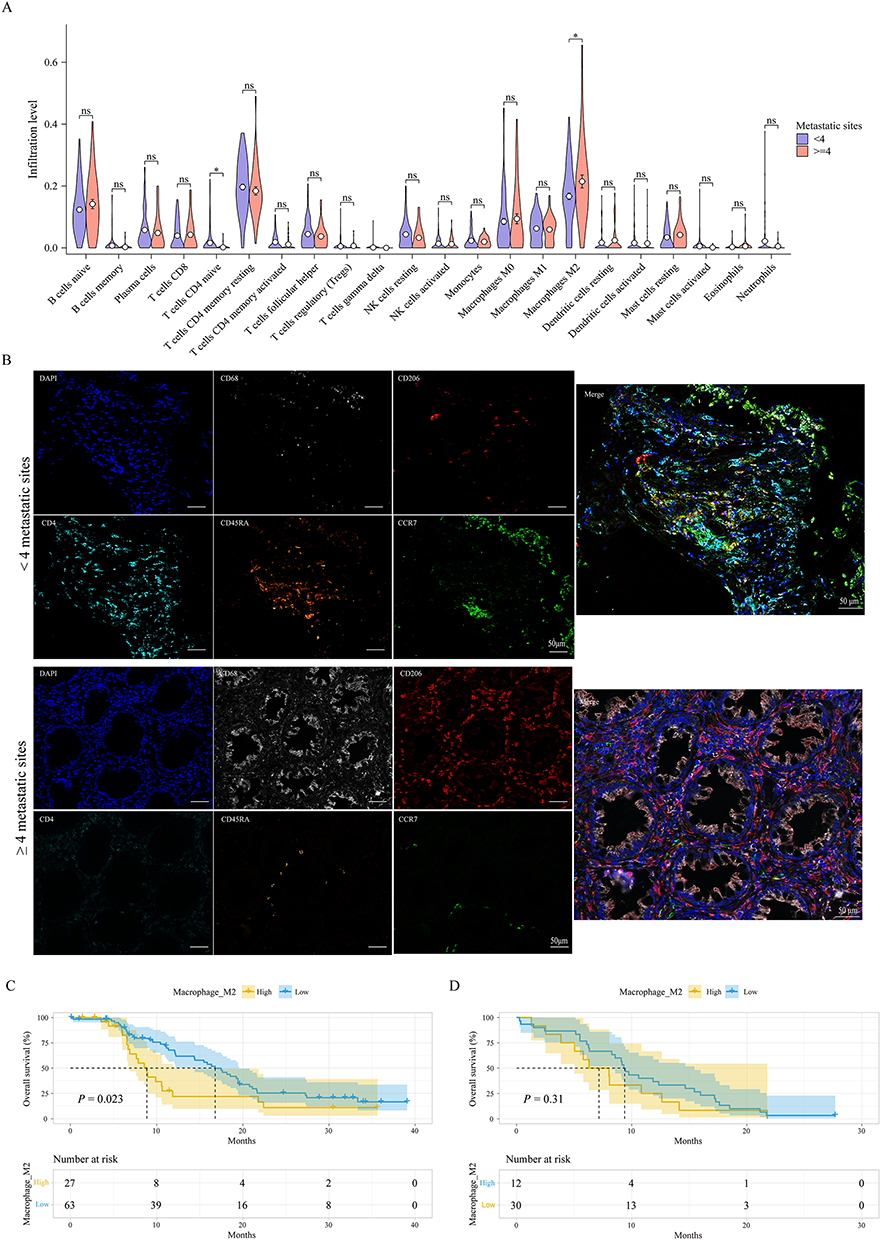 |
Figure 5 The landscape of tumor microenvironment in ES-SCLC patients with ICI treatment. (A) Comparison of tumor immune cells in ES-SCLC patients harboring B) The mIF of M2 macrophage and CD4 naïve T cells in SCLC patients with ICI treatment. The representative images illustrate M2 macrophages stained for CD206 (red) and CD68 (white), alongside the staining of CD4 (light-blue), CD45RA (orange), CCR7 (green), with nuclei colored in dark-blue within SCLC tissues derived from ICI-treated patients. Scales depict sizes of 50μm and 20μm shown in the images. (C) Subgroup survival analysis between M2-macrophage high and M2-macrophage low in ES-SCLC patients harboring high immune infiltration. (D) Subgroup survival analysis between M2-macrophage high and M2-macrophage low in ES-SCLC patients harboring ≥ 4 metastatic sites. *: P compared across these groups.
|
S100A16 May Regulate M2 Macrophage Infiltration in SCLC Patients with Less Than 4 Metastatic Sites
Utilizing data derived from the IMpower133 study, we analyzed significantly altered genes between SCLC patients. SCLC patients from the Shanzhong cohort corroborated higher levels of S100A16 expression in those with at least four metastatic sites compared to those with fewer than four sites. Correlation analysis indicated a negative relationship between S100A16 and CD4 naïve T cells (R = −0.483, P = 0.022). Following this, we investigated the influence of S100A16 expression on overall survival, illuminating the association in SCLC patients with significant survival correlations (P=0.014).
Discussion
The advancements in SCLC treatment achieved through ICI utilization in first-line therapies prompt further examination of the ICI’s role as a retreatment option following first-line therapy failures. Our study uniquely establishes a comparison of survival outcomes in patients with ES-SCLC undergoing second-line treatments incorporating either atezolizumab or alternative anti-cancer therapies. Additionally, we elucidated the differential responses of patients based on the presence or absence of atezolizumab in subgroup analyses, revealing that those with ES-SCLC and fewer than four metastatic sites derive discernible survival benefits from atezolizumab after progression.
Prior investigations have predominantly focused on the efficacy of ICIs as first-line treatments in ES-SCLC. For example, the IMpower133 trial produced compelling results signifying that the integration of atezolizumab with carboplatin and etoposide leads to improved survival in ES-SCLC patients. Ongoing research emphasizes maintaining atezolizumab alongside chemotherapy or alternate ICI treatments to augment survival outcomes.
Our findings indicate a numerical survival advantage for patients with SCLC receiving atezolizumab against those treated with alternative therapies after progression from initial treatment. Nonetheless, evidence of a survival advantage conferred by atezolizumab treatment may be limited in the absence of precise patient stratification in subsequent treatments. Distinct responses may arise among heterogeneous patient subgroups, thus underlining the necessity for identifying atezolizumab-responsive patient populations.
Age is asserted as a substantial predictor impacting resilience to immunotherapy, primarily due to age-related alterations in the immune response. As patients age, innate immune systems promote a chronic inflammatory state while T cell functionality diminishes, impairing the efficacy of immunotherapeutic interventions. Subgroup analyses portrayed superior survival outcomes for treated ES-SCLC patients that possess fewer metastatic sites conducive to positive treatment responses. These insights have significant implications for clinical practice concerning the strategic use of atezolizumab in patients with fewer than four metastatic sites.
Our exploration, therefore, raises critical inquiries regarding the mechanisms through which patients with fewer than four metastatic sites demonstrate enhanced survival benefits from atezolizumab treatment. The TME, a dynamic and complex environment in SCLC, is integral to the metastatic process. Increasing awareness of TME’s role in influencing immune responses highlights its impact on clinical efficacy of immunotherapy. Patient categorization based on TME characteristics delineates “hot” tumors with high immune infiltration from “cold” tumors that lack robust immune responses, with the latter being less responsive to ICIs.
Crucially, the immune context associated with the number and sites of metastatic disease presents an essential consideration in mediating the impact of immunotherapy responses, implicating the significant role of the TME. Variability in the TME can fundamentally alter therapeutic efficacy, given that the presence of diverse immune cells in certain organs fosters antitumor immunity while other sites exhibit immunosuppressive characteristics.
In this study, we noted a positive correlation between S100A16 and M2 macrophage activity while observing a negative association with CD4 naïve T cell activity, suggesting S100A16’s potential role in TME modulation. The interactions among these components merit deeper investigation to elucidate their functional mechanisms within the TME.
While our study presents valuable insights, certain limitations persist. Further subgroup analyses tailored to explore various atezolizumab treatment regimens, such as monotherapy or combination therapies, would strengthen our findings. Additionally, factors influencing the efficacy of immunotherapy not included in our study may render results less definitive.
To the best of our knowledge, we provide the first evidence that patients harboring fewer than four metastatic sites in ES-SCLC may stand to benefit significantly from ICI rechallenge.
Data Sharing Statement
The data supporting the findings of this study are available upon request from the corresponding authors.
Acknowledgments
Funding
This study was funded by the Special Funds for Taishan Scholars Project (Grant No. tsqn201812149), the Academic promotion program of Shandong First Medical University (2019RC004), and the National Natural Science Foundation of China (No. 82003996).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Jackman DM, Johnson BE. Small-cell lung cancer. Lancet. 2005;366(9494):1385–1396. doi:10.1016/S0140-6736(05)67569-1
2. Wang S, Zimmermann S, Parikh K, et al. Current diagnosis and management of small-cell lung cancer. Mayo Clin Proc. 2019;94(8):1599–1622. doi:10.1016/j.mayocp.2019.01.034
3. Lahiri A, Maji A, Potdar PD, et al. Lung cancer immunotherapy: progress, pitfalls, and promises. Mol Cancer. 2023;22(1):40. doi:10.1186/s12943-023-01740-y
4. Facchinetti F, Di Maio M, Tiseo M. Adding PD-1/PD-L1 inhibitors to chemotherapy for the first-line treatment of extensive stage small cell lung cancer (SCLC): a meta-analysis of randomized trials. Cancers. 2020;12(9):2645. doi:10.3390/cancers12092645
5. Horn L, Mansfield AS, Szczęsna A; IMpower133 Study Group, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. doi:10.1056/NEJMoa1809064
6. Paz-Ares L, Dvorkin M, Chen Y; CASPIAN investigators, et al. Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomized, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929–1939. doi:10.1016/S0140-6736(19)32222-6
7. Melosky B, Cheema PK, Brade A, et al. Role of immune checkpoint inhibitors in the treatment of ES-SCLC. Oncologist. 2020;25(11):981–992. doi:10.1634/theoncologist.2020-0193
8. Kuczynski EA, Sargent DJ, Grothey A, et al. Drug rechallenge and treatment beyond progression–implications for drug resistance. Nat Rev Clin Oncol. 2013;10(10):571–587. doi:10.1038/nrclinonc.2013.158
9. Keenan TE, Burke KP, Van Allen EM. Genomic correlates of response to immune checkpoint blockade. Nat Med. 2019;25(3):389–402. doi:10.1038/s41591-019-0382-x
10. Watanabe H, Kubo T, Ninomiya K, et al. The effect and safety of immune checkpoint inhibitor rechallenge in non-small cell lung cancer. Jpn J Clin Oncol. 2019;49(8):762–765. doi:10.1093/jjco/hyz066
12. Cabezas-Camarero S, Cabrera-Martín MN, Pérez-Segura P. Response to immunotherapy rechallenge after interval chemotherapy in a patient with head and neck cancer. Anticancer Drugs. 2019;30(2):149–152. doi:10.1097/CAD.0000000000000706
13. Zhang Z, Li Y, Dong Y, et al. Successful treatment of a patient with multiple-line relapsed extensive-stage small-cell lung cancer receiving penpulimab combined with anlotinib: a case report. Front Oncol. 2022;12:846597. doi:10.3389/fonc.2022.846597
14. Fridman WH, Zitvogel L, Sautès-Fridman C, et al. The immune contexture in cancer prognosis and treatment. Nat Rev Clin Oncol. 2017;14(12):717–734. doi:10.1038/nrclinonc.2017.101
15. Murciano-Goroff YR, Warner AB, Wolchok JD. The future of cancer immunotherapy: microenvironment-targeting combinations. Cell Res. 2020;30(6):507–519. doi:10.1038/s41422-020-0337-2
16. Liu YT, Sun ZJ. Turning cold tumors into hot tumors by improving T-cell infiltration. Theranostics. 2021;11(11):5365–5386. doi:10.7150/thno.58390
17. Iglesias-Escudero M, Arias-González N, Martínez-Cáceres E. Regulatory cells and the effect of cancer immunotherapy. Mol Cancer. 2023;22(1):26. doi:10.1186/s12943-023-01714-0
18. Chen B, Khodadoust MS, Liu CL, et al. Profiling tumor infiltrating immune cells with CIBERSORT. Methods Mol Biol. 2018;1711:243–259.
19. Hazra A, Gogtay N. Biostatistics series module 4: comparing groups – categorical variables. Indian J Dermatol. 2016;61(4):385–392. doi:10.4103/0019-5154.185700
20. El Sayed R, Blais N. Immunotherapy in extensive-stage small cell lung cancer. Curr Oncol. 2021;28(5):4093–4108. doi:10.3390/curroncol28050347
21. Barrows ED, Blackburn MJ, Liu SV. Evolving role of immunotherapy in small cell lung cancer. Semin Cancer Biol. 2022;86(Pt 3):868–874. doi:10.1016/j.semcancer.2022.02.021
22. Reck M, Mok TSK, Mansfield A, et al. Brief report: exploratory analysis of maintenance therapy in patients with extensive-stage SCLC treated first line with atezolizumab plus carboplatin and etoposide. J Thorac Oncol. 2022;17(9):1122–1129. doi:10.1016/j.jtho.2022.05.016
23. Spigel DR, Vicente D, Ciuleanu TE, et al. Second-line nivolumab in relapsed small-cell lung cancer: CheckMate 331☆. Ann Oncol. 2021;32(5):631–641. doi:10.1016/j.annonc.2021.01.071
24. Pujol JL, Greillier L, Audigier-Valette C, et al. A randomized non-comparative phase II study of anti-programmed cell death-ligand 1 atezolizumab or chemotherapy as second-line therapy in patients with small cell lung cancer: results from the IFCT-1603 trial. J Thorac Oncol. 2019;14(5):903–913. doi:10.1016/j.jtho.2019.01.008
26. Granier C, Gey A, Roncelin S, et al. Immunotherapy for older cancer patients. Biomed J. 2021;44(3):260–271. doi:10.1016/j.bj.2020.07.009
27. Kaiser M, Semeraro MD, Herrmann M, et al. Immune aging and immunotherapy in cancer. Int J Mol Sci. 2021;22(13):7016. doi:10.3390/ijms22137016
28. Li T, Qiao T. Unraveling the tumor microenvironment in small-cell lung cancer: implications for immunotherapy. Semin Cancer Biol. 2022;86(Pt 2):117–125. doi:10.1016/j.semcancer.2022.09.005
29. Khan P, Fatima M, Khan MA, et al. Emerging role of chemokines in small cell lung cancer. Semin Cancer Biol. 2022;87:117–126. doi:10.1016/j.semcancer.2022.11.005
30. Niu X, Chen L, Li Y, et al. Ferroptosis and necroptosis in the tumor microenvironment: their perspectives in SCLC immunotherapy. Semin Cancer Biol. 2022;86(Pt 3):273–285. doi:10.1016/j.semcancer.2022.03.009
31. Caliman E, Fancelli S, Petroni G, et al. Challenges in treating small cell lung cancer in the immunotherapy era. Lung Cancer. 2023;175:88–100. doi:10.1016/j.lungcan.2022.11.014
32. Gay CM, Stewart CA, Park EM, et al. Patterns of transcription factor programs define key subtypes of SCLC with therapeutic vulnerabilities. Cancer Cell. 2021;39(3):346–360. doi:10.1016/j.ccell.2020.12.014
33. Makrakis D, Talukder R, Lin GI, et al. Association between the sites of metastasis and outcomes with immune checkpoint inhibitors. Clin Genitourin Cancer. 2022;20(5):e440–e452. doi:10.1016/j.clgc.2022.06.001
34. Yu J, Green MD, Li S, et al. Impact of liver metastasis on immunotherapy efficacy via macrophage-mediated T cell elimination. Nat Med. 2021;27(1):152–164. doi:10.1038/s41591-020-1131-x
35. Quail DF, Joyce JA. The regulatory role of microenvironments in tumor progression and metastasis. Nat Med. 2013;19(11):1423–1437. doi:10.1038/nm.3394
36. Christofides A, Strauss L, Yeo A, et al. The complex roles of tumor-infiltrating macrophages. Nat Immunol. 2022;23(8):1148–1156. doi:10.1038/s41590-022-01267-2
37. Gordon SR, Maute RL, Dulken BW, et al. PD-1 expression by tumor-associated macrophages inhibits phagocytosis and immunity. Nature. 2017;545(7655):495–499. doi:10.1038/nature22396
38. Kim YJ, Won CH, Lee MW, et al. Correlation between tumor-associated macrophage activity and relevant immune checkpoint molecules in cutaneous melanoma. J Clin Med. 2020;9(8):2500. doi:10.3390/jcm9082500
39. Iriki T, Ohnishi K, Fujiwara Y, et al. The interactions between tumor-associated macrophages and SCLC cells are involved in tumor progression via STAT3 activation. Lung Cancer. 2017;106:22–32. doi:10.1016/j.lungcan.2017.01.003
40. Zhang Q, Sioud M. Tumor-associated macrophage subsets: shaping polarization and targeting. Int J Mol Sci. 2023;24(8):7493. doi:10.3390/ijms24087493
41. Borst J, Ahrends T, Bąbała N, et al. CD4+ T cell assistance in tumor immunology and therapy. Nat Rev Immunol. 2018;18(10):635–647. doi:10.1038/s41577-018-0044-0
Welcome to the Wild World of Cancer Research!
Okay folks, buckle up, because we’re diving into the riveting realm of small cell lung cancer (SCLC). Now, before you roll your eyes and start scrolling through cat memes on your phone, let’s remember that this is serious stuff—but hey, I promise to keep it entertaining. So, settle in, and let’s see if we can find the silver lining in the rather grim cloud that is extensive-stage small cell lung cancer (ES-SCLC).
First Things First: What on Earth Are We Talking About?
Our intrepid researchers set out with a mission: to explore if a cheeky little thing called ICI rechallenge could actually improve survival for patients who have already been put through the wringer of first-line therapy. Picture this: you battle through treatment only to think, “What if I could have another go at the very thing that frustrated me the first time?” Well, that’s the crux of ICI rechallenge, and they weren’t just asking for a second date; they wanted to investigate if the tumor microenvironment (TME)—that delightful little ecosystem where all the cancer magic happens—could be coaxed into a better relationship with our immune system. Who knew tumors could be so complicated?
Data Galore: The Study that Might Just Save Lives
The team relied on the IMpower133 study and a whole load of data from the Shandong Cancer Hospital—sounds impressive, right? They had a randomized, double-blind, Phase I/III study that didn’t just show results; it practically paraded them around in a sparkly outfit, demonstrating significant improvements in overall and progression-free survival. In simpler terms: adding atezolizumab to treatment helped patients live longer—not to mention with a bit of pizzazz!
Immune Cell Dancers of the TME
We all have that friend who brings the party, and in our case, those friends are the immune cells infiltrating the TME. The team utilized a technical whizz called CIBERSORT (isn’t that a great name?) to estimate the proportions of 22 immune cell types in the SCLC specimens! Think of them as the cast of an epic battle, each with their own unique strengths and weaknesses. From B cells to macrophages, they were all marching to a different beat in the fight against cancer.
Oh, the Numbers!
In total, there were 201 SCLC patients strutting their stuff. After some selective pruning of the data tree (97 patients gracefully exited stage left for various reasons), we were left with some serious contenders: 54 were treated with atezolizumab after the first round, while 71 opted for other anti-cancer therapies. A veritable reality TV show of treatment choices!
Statistical Analysis: More Than Just Number Crunching
They did what any good researcher might do: they crunched numbers, made charts, and tried to find significant differences—think of it as an academic version of “Where’s Waldo?” The results suggested a noteworthy pattern where those treated with atezolizumab had longer survival, especially in patients with less than four metastatic sites. In other words, location, location, location—the cancer landscape matters!
Let’s Talk Survival Rates
Ready for the good news? If you were one of those lucky patients with fewer than four metastatic sites, you might just find yourself benefitting from a rechallenge with atezolizumab. The survival curves proved it: the less complicated your cancer’s address, the better your chances after taking another swing at ICI treatment. This begs the question: could we be on the cusp of redefining how we approach treatment for patients with SCLC?
But Wait, There’s More!
The implications of this study are vast, hinting that we might be onto something big. Now, this isn’t just theoretical; there’s a practical element here too. The researchers proposed that the key to survival benefits lies in reshaping the TME. It’s like turning an unkempt garden into a blooming wonderland—less chaos, more flowers. And if that’s true, we’re all for it!
The Future of ES-SCLC Treatment
So what’s the takeaway? Well, while the researchers are excited about the findings, they also acknowledge the needs for further studies. And let’s be honest, in the world of cancer research, there’s always room for improvement and exploration. As they say, “Rome wasn’t built in a day.” But who knows, with more research and a sprinkle of good luck, maybe we’ll find ourselves with even more effective treatment strategies for ES-SCLC.
In Conclusion: A Moment of Reflection
As I wrap up this entertaining tour-de-force through the complex world of cancer treatment, let’s remember the real heroes: the patients battling this disease. Research like this brings hope, and if we can unlock even a fraction of this mystery, perhaps we’ll pave the way for more victories in the oncology battlefield. Now, carry on, dear readers, and remember—always keep fighting.
Stay cheeky, stay informed, and here’s to a future where we kick cancer to the curb!
How’s that for keeping it sharp, observational, and just a tad cheeky? Let’s go take on cancer, one witticism at a time!
Chances of enjoying a longer life post-treatment! Specifically, patients who had fewer metastatic sites showed a significant improvement in both overall and progression-free survival rates when treated with the immune checkpoint inhibitor (ICI) in question. It’s like finding a hidden treasure in the battlefield of cancer—location, it seems, is everything.
What’s Next in Our Cancer Adventure?
As we ride the wave of these findings, you might be wondering about the implications. The research suggests that the current strategy of rechallenging with ICIs like atezolizumab, especially in patients with manageable metastatic disease, opens the door to new potential therapies. After all, if we can coax the immune system to better recognize and fight off these pesky cancer cells, who knows what breakthroughs lie ahead?
The Road Ahead: Caution But Hope!
While the results are promising, it’s important to remember a few things. First off, this isn’t a blanket solution for every patient out there. As with many things in medicine, the response to treatment can be wildly varied—sort of like how everyone has a different opinion on pineapple on pizza. There’s a lot to consider—patient health, specific cancer characteristics, and, of course, the quality of the TME.
As we edge toward the horizon of cancer treatment, the focus on personalized medicine continues to rise. Enhancing our understanding of individual responses, the socio-economic factors at play, and the tumors’ unique characteristics will be crucial in designing treatments that truly work.
A Final Thought: The Power of Community
In this long journey through cancer research, it’s vital to recognize the collective effort of researchers, clinicians, and patients. Each data point represents a life, a story, and a possibility of hope. The more we share this knowledge—be it through journals, conferences, or lively discussions—the nearer we inch toward breakthroughs that can change the game for SCLC and other formidable foes in the world of oncology.
So, let’s keep pushing the envelope, educating ourselves and each other, and championing the fighters in this “wild world” of cancer research. Until next time, stay curious, stay informed, and together let’s explore the possibilities!
S. First, this data is just a stepping stone; further studies are crucial to substantiate these findings and refine treatment strategies. Cancer research is often a complex journey filled with unexpected twists and turns, and while we are optimistic, we must also approach these results with a healthy dose of caution.
Moreover, the variations in individual responses mean that personalized treatment plans will be essential. After all, every cancer patient is unique, and the solution that works wonders for one individual might not have the same effect on another. Thus, ongoing research should focus on biomarker identification and personalized medicine approaches to tailor therapies effectively.
Call to Arms!
For all the stakeholders in the cancer community—patients, researchers, and healthcare professionals—staying informed and engaged in this ongoing dialogue is key. Sharing knowledge, supporting clinical trials, and advocating for research funding may hasten the day when we have more effective and accessible treatment options for all cancer patients, including those battling small cell lung cancer.
One Final Note
As we conclude this captivating exploration of small cell lung cancer—from the promising role of immunotherapy to the complexities of the tumor microenvironment—it’s essential to recognize the fight against cancer is relentless and ongoing. There is a sense of camaraderie and hope among researchers and patients alike, and with every study, we edge closer to a future where victories over cancer are more frequent and meaningful. So, let’s stay hopeful, stay informed, and together, let’s march onward in this remarkable journey!
And remember, while we tackle the serious business of science with sincerity, it’s perfectly acceptable to sprinkle a bit of humor into the mix. After all, laughter may just be the best medicine we can offer to ourselves as we navigate the roller coaster of cancer research!

