
How do you distinguish pericardial tamponade from pericardial effusion? Even at 3 a.m., emergency medical professionals must make decisions within minutes before obstructive shock occurs.
This article is not – and this is important – regarding the acute one Pericardtamponade. That means: an echocardiographically representable Pericarderguss and concomitant hemodynamic instability. This situation is usually always to be evaluated as a pericardial tamponade, which requires immediate Pericardiocentesis needed. In this context, it is particularly important to consider that in the case of an acute pericardial tamponade (e.g. following trauma), even the smallest effusion (~ 50mL) can be sufficient for haemodynamic instability. In contrast to subacute tamponades, the pericardium does not have time to expand here.
There is a nice graphical representation of this Ivens et al.
| follow that 12-Channel for more cardiology topics. consequences Are you also interested in news from other medical fields? Discover here other DocCheck channels. |
The clock is ticking
Instead, this article is regarding the minutes, and possibly hours, before obstructive shock occurs. Where emergency physicians have to decide whether it is a case of subacute pericardial tamponade or pericardial effusion – in the spirit of Felix’s lecture on periarrest situations. A special focus is always that the tricks work without any problems even at 3 a.m.
Subacute pericardial tamponades are usually associated with a rather chronic course. The pericardium can stretch and even compensate for large effusions of 1-2 l. But only up to the point in time X when the pericardium can no longer expand and even a small, further increase in fluid leads to pericardial tamponade. The diagnostic criteria for pericardial tamponade are not uniform, so the information on the sensitivity and specificity of the individual echocardiographic findings should be treated with caution.
Since it cannot be mentioned often enough, the disclaimer once more: A pericardial effusion with simultaneous hemodynamic instability is generally to be evaluated as a pericardial tamponade and requires one Pericardiocentesis!
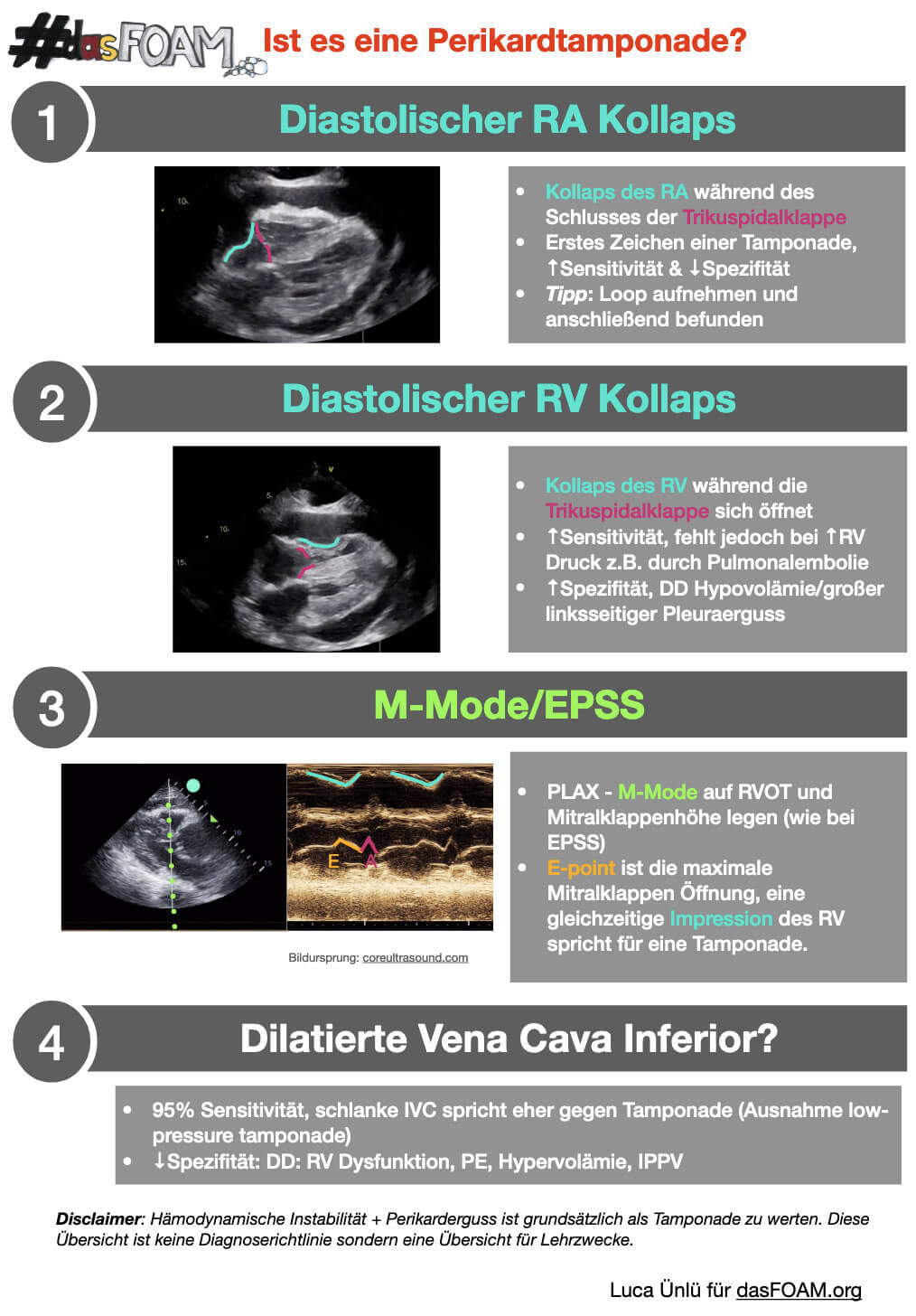 Is it a pericardial tamponade? Credit: dasFOAM
Is it a pericardial tamponade? Credit: dasFOAM
Systolic or diastolic?
All information on sensitivity and specificity were taken from the Narrative Reviewwhich 2018 in American Journal of Emergency Medicine has been published. Strong reading recommendation – almost all recent resources on the topic of pericardial tamponade in emergency medicine refer to this review. In May 2022 will appear in the American Journal of Emergency Medicine an even more extensive one Review by the same group of authors.
One point that can cause some confusion is the “systolic RA collapse” which we also like coreultrasound.com Call it “diastolic RA collapse” because at the end of the Tricuspid valve the right atrium is in diastole and the right ventricle is in systole. Because when the atrium is in systole, a collapse of the right atrium (RA) can actually always be shown by echocardiography – since it empties into the right ventricle (RV).
Image source: Paige Codyunsplash

