

Introduction
Diabetes remains one of the most pressing public health crises globally, impacting approximately 451 million individuals as of 2017. Projections indicate that this figure could surge to as high as 693 million by 2045.1 The widespread occurrence of diabetes-related chronic complications considerably reduces both the life quality and life expectancy of those affected.2 Among these complications, diabetic peripheral neuropathy (DPN) is notably prevalent, afflicting around 50% of diabetes patients, regardless of whether they have type 1 or type 2 diabetes.3
Diabetic Peripheral Neuropathy (DPN) may lead to debilitating symptoms such as numbness and pain in the legs and feet, serious complications like foot ulcers, and in severe cases, the need for limb amputation. These issues can drastically reduce a patient’s overall quality of life. The development of DPN often progresses slowly and insidiously, resulting in as many as 50% of individuals showing no symptoms in the early stages, contributing to oversight and delayed treatment. This underscores the critical need for timely recognition and preventive measures concerning diabetic peripheral neuropathy.4 The mechanisms behind DPN are complex and involve several factors, such as oxidative stress, inflammatory responses, and neurotrophic dysregulation.5–7 Research by Wahren et al.8 suggested that administration of C-peptide analogues yielded significant improvements in vibration perception thresholds compared to placebo, hinting at the potential of C-peptide replacement therapy to enhance neurological function in DPN patients. C-peptide, a stable byproduct of glucagon secretion, is a critical biomarker for assessing pancreatic islet function.9 Additionally, findings from Umaid Potaliya et al.10 indicated a strong correlation between decreased serum C-peptide levels and the occurrence of DPN among individuals with type 2 diabetes, highlighting an increased risk of DPN with longer diabetes durations.11 Notably, research has revealed that physiological levels of C-peptide exhibit anti-inflammatory, immunomodulatory, and neurotrophic properties, with studies noting that C-peptide and its derivatives can effectively lower blood glucose levels and mitigate diabetes complications.12 Currently, no extensive investigations have explored the association between fasting C-peptide/diabetes duration (FCP/DD) and type 2 diabetes coexisting with DPN. This study intends to analyze the interrelation between the FCP/DD ratio and the incidence of diabetic peripheral neuropathy within the context of type 2 diabetes. The goal is to identify a novel clinical marker for the early detection and prognostic evaluation of DPN.
Methods
Subjects
For this study, a cohort of 816 patients diagnosed with type 2 diabetes and admitted to Hebei Provincial People’s Hospital in 2022 was analyzed. The inclusion criteria adhered to the diagnostic standards established by the World Health Organization (WHO) in 1999. Exclusion criteria encompassed: (1) cases of type 1 diabetes, gestational diabetes, or other special diabetes types; (2) individuals aged 80 years and older; (3) admissions associated with acute diabetes complications such as ketoacidosis, hyperosmolar-hyperglycemic state, or hypoglycemic coma; (4) historical cases of type B viral hepatitis, cirrhosis, hepatic encephalopathy, or prior liver surgery; (5) recent severe comorbidities including renal dysfunction, cardiovascular issues, infections, tumors, or blood disorders; (6) periods of pregnancy or lactation; (7) neuropathy due to other underlying conditions or pharmacotherapy; and (8) neurotoxicity from medications. Symptoms related to neuropathy, such as burning sensations, numbness, and fatigue, were assessed alongside objective neurological signs, including sensitivity to vibration, pain, and reflex actions. The abnormalities detected in the symptoms and signs indicative of DPN followed a glove and stocking distribution pattern. The Toronto Clinical Scoring System (TCSS) and neurophysiological assessments were utilized as diagnostic benchmarks to validate DPN.13 Specifically, participants were categorized as: (1) non-DPN, where all neurophysiological evaluations yielded normal results; (2) clinically diagnosed DPN, indicated by at least two abnormal results in neurological assessments or ankle reflex evaluation, despite normal nerve conduction velocities (NCV); (3) confirmed DPN, characterized by anomaly in at least one nerve conduction parameter across two or more specific nerves, regardless of neurological signs or symptoms. Ethical clearance for this research was granted by the Ethics Committee of Hebei Provincial People’s Hospital, ensuring patient anonymity and confidentiality, exempting the requirement for signed informed consent.
Data Collection and Laboratory Analysis
Data encompassing general and biochemical parameters were meticulously gathered: demographic details such as gender, age, duration of diabetes, and histories regarding smoking, alcohol consumption, hypertension, fatty liver disease, diabetic nephropathy, and retinopathy. Body measurements including height and weight were documented, enabling the calculation of body mass index (BMI). Blood samples were collected under fasting conditions following an 8-10 hour period post-admission, with assessments made for white blood cell counts, neutrophil percentages, albumin levels, fasting blood glucose, glycated hemoglobin, and various cholesterol types. Comprehensive laboratory analyses were facilitated using flow cytometry for routine blood checks, automatic biochemical analyzers for biochemical assessments, and high-performance liquid chromatography for glycated hemoglobin evaluation, along with electrochemiluminescence techniques for fasting C-peptide determination. All lab procedures were performed by qualified laboratory technicians.
Calculation of Ratio and Grouping
The Fasting C-peptide/Diabetes Duration (FCP/DD) ratio was computed by dividing fasting C-peptide levels by diabetes duration. This ratio’s median was statistically determined to be 0.25, and based on this threshold, patients were allocated into two distinct groups: the Low FCP/DD group (FCP/DD≤0.25, n=408) and the High FCP/DD group (FCP/DD >0.25, n=408). Participants with type 2 diabetes were further subdivided into the DPN group (n=455) and the non-DPN (NDPN) group (n=361), contingent on the presence or absence of diabetic peripheral neuropathy.
Statistical Methods
Data analysis was performed using SPSS 25.0 software. Normal distribution measurement data were expressed as mean ± standard deviation, applying two independent sample t-tests for group comparisons. For non-normal data, results were presented as median with interquartile ranges [M(P25%, P75%)], utilizing the Mann–Whitney U test for comparisons. Categorical variables were presented in percentage formats, with the chi-square test employed for intergroup comparisons. The relationships between continuous variables were explored using Pearson’s correlation when normality assumptions held, and Spearman’s rank correlation for non-normally distributed data. A binary logistic regression analysis identified DPN determinants. The predictive abilities of fasting C-peptide (FCP), diabetes duration (DD), and the FCP/DD model for DPN were evaluated using Receiver Operating Characteristic (ROC) curve analysis, including area under the curve (AUC) calculations. The DeLong test was implemented for AUC comparison, and significance was determined at a p-value of <0.05.
Results
Comparison of General Data and Laboratory-Related Indicators in All Patients
A total of 816 patients with T2DM were included in this study, including 455 patients (55.76%) with DPN and 361 patients (44.24%) with NDPN. The differences in age, diabetes duration, the proportion of history of combined fatty liver, FCP/DD, GFR, and fasting C-peptide were statistically significant between the two groups of study subjects (P 0.05) (Table 1).
|
|
Comparison of General Data and Laboratory-Related Indicators on Study Participants from Different FCP/DD Subgroups
The age, diabetes duration, the proportion of history of combined hypertension, proportion of combined diabetic peripheral neuropathy, proportion of combined diabetic nephropathy, and proportion of combined diabetic retinopathy, HDL-C, and NEUT in the High FCP/DD group were lower than those in the Low FCP/DD group (P C, ESR, Cr, and WBC between the two study groups was not statistically significant (Table 2).
 |
|
Correlation Analysis Between FCP/DD and Indicators
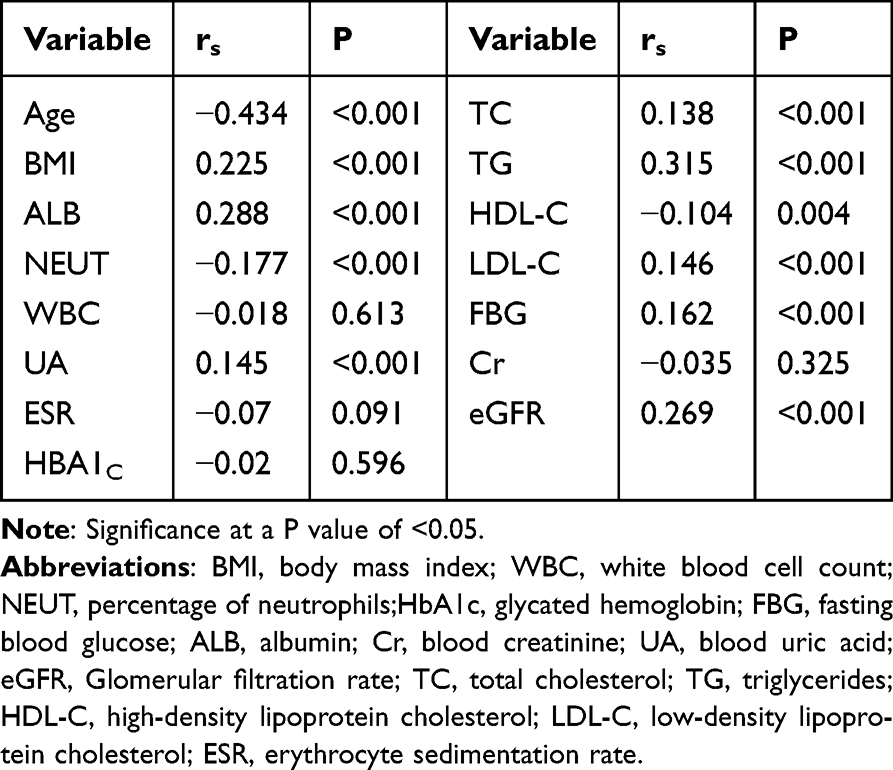 |
Table 3 Correlation Analysis Between FCP/DD and Indicators (Rs Value)
|
Multifactor Logistic Regression Analysis of FCP/DD on DPN
In our analysis considering whether T2DM was compounded by DPN, we filtered clinical data and biochemical indicators to include only independent variables. The analysis indicated a high FCP/DD ratio acted as a protective factor against DPN risk.Table 4
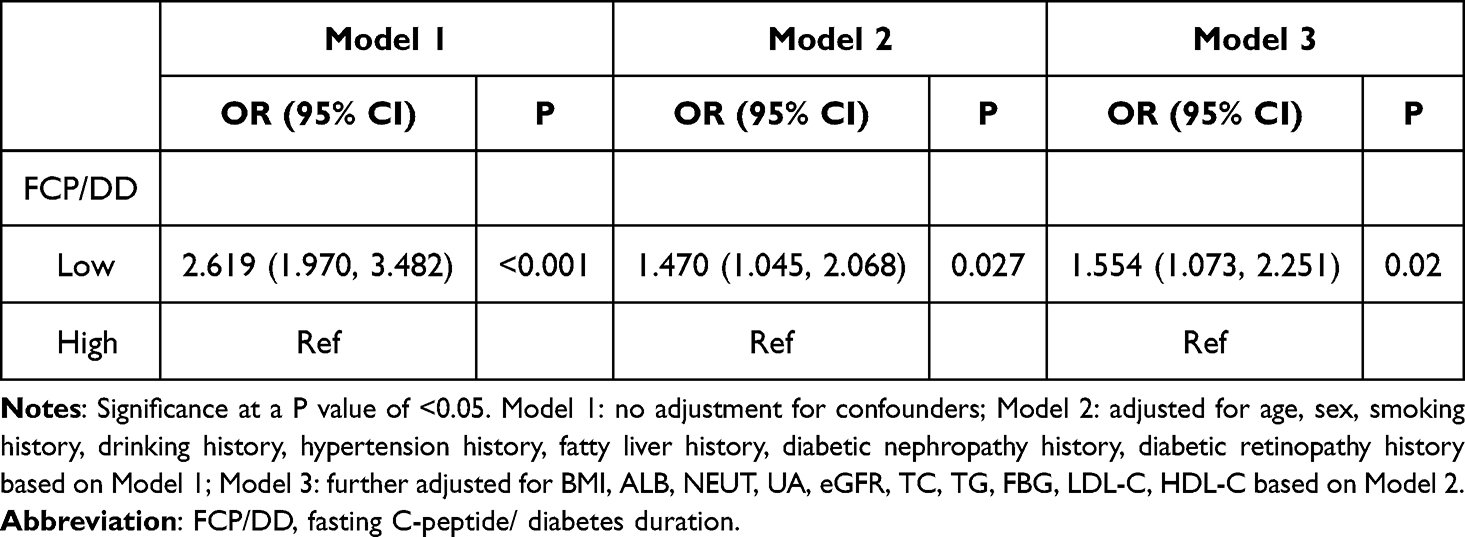 |
Table 4 Multifactor Logistic Regression Analysis of FCP/DD on DPN
|
Evaluate the Predictive Value of FCP, DD, and the FCP/DD Model for T2DM with DPN and Compare Using the DeLong Test
The regression equation illustrates the relationship between variables, indicating how FCP, DD, and the FCP/DD ratio contribute to predicting DPN occurrence. The AUC analysis demonstrated that the predictive capacity of the FCP/DD model surpassed both FCP and DD individually, establishing the FCP/DD ratio as a key clinical indicator in assessing DPN risk.Table 5
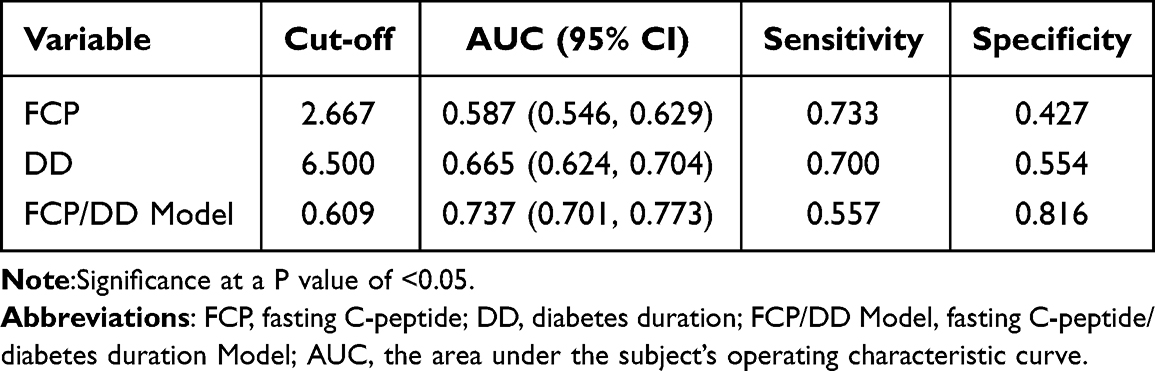 |
Table 5 ROC Curves of FCP, DD, and FCP/DD Model
|
Discussion
Diabetic peripheral neuropathy (DPN) poses significant diagnostic challenges due to the subtlety of early fibrotic lesion identification, which often postpones necessary intervention until clinical manifestations arise. The resulting delays can culminate in dire consequences, such as ulcer formation or elevated risks of limb amputation, which ultimately lead to irreversible neuropathic damage.14 Therefore, it is crucial to understand early indicators or predictive markers for DPN, especially in light of inadequate treatment strategies that could greatly enhance patient quality of life.
Our investigation revealed that individuals with DPN commonly presented advanced age, prolonged diabetes duration, higher instances of hypertension, and increased rates of diabetic complications, corroborated by findings from Wang et al.4. Correlations between DPN development and histories of both diabetic nephropathy and retinopathy were also identified.15 While fasting blood glucose levels and glycated hemoglobin showed no meaningful statistical differences among various subpopulations, it may reflect the tight glycemic control achieved via standardized therapeutic regimens. Additionally, our analysis yielded consistently non-significant outcomes regarding gender’s influence on DPN susceptibility, aligning with earlier studies indicating no notable gender correlation.16
Moreover, we scrutinized the utility of the FCP/DD ratio as a predictor for DPN. The robustness of our ROC curve analysis highlighted that the FCP/DD ratio offered superior predictive capability over either fasting C-peptide or diabetes duration alone, solidifying its role as a clinical tool in assessing DPN risk.
Conclusion
In summary, a high FCP/DD ratio represents a significant protective factor against the combined effects of type 2 diabetes and DPN. The FCP/DD model demonstrates considerable predictive validity for identifying patients at risk for DPN, proving its clinical relevance beyond using FCP or DD independently.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki principles and received approval from the Ethical Committees of Hebei General Hospital (No.2024-LW-145). Given the retrospective non-interventional design, patient anonymity was maintained, and informed consent was deemed unnecessary.
Funding
This study was not financed by any external funding sources.
Disclosure
No conflicts of interest were disclosed by the authors regarding this research.
References
1. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790. doi:10.1038/s41598-020-71908-9
2. Li Y, Li Y, Deng N, Shi H, Caika S, Sen G. Training and external validation of a predict nomogram for type 2 diabetic peripheral neuropathy. Diagnostics. 2023;13(7):1265. doi:10.3390/diagnostics13071265
3. Yan P, Wu Y, Dan X, et al. Aspartate aminotransferase/alanine aminotransferase ratio was associated with type 2 diabetic peripheral neuropathy in a Chinese population: a cross-sectional study. Front Endocrinol (Lausanne). 2023;14:1064125. doi:10.3389/fendo.2023.1064125
4. Wang W, Ji Q, Ran X, et al. Prevalence and risk factors of diabetic peripheral neuropathy: a population-based cross-sectional study in China. Diabetes Metab Res Rev. 2023;39(8):e3702. doi:10.1002/dmrr.3702
5. Azoulay D, Abed S, Sfadi A, et al. Low brain-derived neurotrophic factor protein levels and single-nucleotide polymorphism Val66Met are associated with peripheral neuropathy in type II diabetic patients. Acta Diabetol. 2020;57(7):891–898. doi:10.1007/s00592-020-01508-6
6. Mallet ML, Hadjivassiliou M, Sarrigiannis PG, Zis P. The role of oxidative stress in peripheral neuropathy. J Mol Neurosci. 2020;70(7):1009–1017. doi:10.1007/s12031-020-01495-x
7. Ristikj-Stomnaroska D, Risteska-Nejashmikj V, Papazova M. Role of inflammation in the pathogenesis of diabetic peripheral neuropathy. Open Access Maced J Med Sci. 2019;7(14):2267–2270. doi:10.3889/oamjms.2019.646
8. Wahren J, Foyt H, Daniels M, Arezzo JC. Long-acting c-peptide and neuropathy in type 1 diabetes: a 12-month clinical trial. Diabetes Care. 2016;39(4):596–602. doi:10.2337/dc15-2068
9. Qin J, Sun R, Ding D. Effects of serum C-peptide level on blood lipid and cardiovascular and cerebrovascular injury in patients with type 2 diabetes mellitus: a meta-analysis. Contrast Media Mol Imaging. 2022;2022(1):6314435. doi:10.1155/2022/6314435
10. Potaliya U, Tak S, Goyal M. Association of C-peptide level with peripheral neuropathy in type 2 diabetes: an observational cross-sectional preliminary study. Diabetes Metab Syndr. 2023;17(2):102725. doi:10.1016/j.dsx.2023.102725
11. Li C, Wang W, Ji Q, et al. Prevalence of painful diabetic peripheral neuropathy in type 2 diabetes mellitus and diabetic peripheral neuropathy: a nationwide cross-sectional study in mainland China. Diabet Res Clin Pract. 2023;198:110602. doi:10.1016/j.diabres.2023.110602
12. Pathan R, Purohit N, Choudhary P. Study of serum C-peptide levels in newly diagnosed diabetic mellitus subjects of North Gujarat region of India. Int J Adv Med. 2022;9(2):142. doi:10.18203/2349-3933.ijam20220124
13. Tesfaye S, Boulton AJ, Dyck PJ, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments [published correction appears in Diabetes Care. 2010 Dec; 33(12):2725]. Diabetes Care. 2010;33(10):2285–2293. doi:10.2337/dc10-1303
14. Lian X, Qi J, Yuan M, et al. Study on risk factors of diabetic peripheral neuropathy and establishment of a prediction model by machine learning. BMC Med Inform Decis Mak. 2023;23(1):146. doi:10.1186/s12911-023-02232-1
15. Yang J, Jiang S. Development and validation of a model that predicts the risk of diabetic nephropathy in type 2 diabetes mellitus patients: a cross-sectional study. Int J Gen Med. 2022;15:5089–5101. doi:10.2147/IJGM.S363474
16. Dinh Le T, Phi Thi Nguyen N, Thanh Thi Tran H, et al. Diabetic peripheral neuropathy associated with cardiovascular risk factors and glucagon-like peptide-1 concentrations among newly diagnosed patients with type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2022;15:35–44. doi:10.2147/DMSO.S344532
17. Qiao X, Zheng H, Zhang S, et al. C-peptide is independent associated with diabetic peripheral neuropathy: a community-based study. Diabetol Metab Syndr. 2017;9(1):12. doi:10.1186/s13098-017-0208-2
19. Zhao L, Ma J, Wang S, et al. Relationship between β-cell function, metabolic control, and microvascular complications in type 2 diabetes mellitus. Diabetes Technol The. 2015;17(1):29–34. doi:10.1089/dia.2014.0214
20. Ekberg K, Johansson BL. Effect of C-peptide on diabetic neuropathy in patients with type 1 diabetes. Exp Diabetes Res. 2008;2008(1):457912. doi:10.1155/2008/457912
21. Elafros MA, Andersen H, Bennett DL, et al. Towards prevention of diabetic peripheral neuropathy: clinical presentation, pathogenesis, and new treatments. Lancet Neurol. 2022;21(10):922–936. doi:10.1016/S1474-4422(22)00188-0
22. Li J, Zhang X, Zhang Y, et al. Increased systemic immune-inflammation index was associated with type 2 diabetic peripheral neuropathy: a cross-sectional study in the Chinese population. J Inflamm Res. 2023;16:6039–6053. doi:10.2147/JIR.S433843
23. Ban J, Pan X, Yang L, et al. Correlation between fibrinogen/albumin and diabetic peripheral neuropathy. Diabetes Metab Syndr Obes. 2023;16:2991–3005. doi:10.2147/DMSO.S427510
Welcome to Diabetic Drama: Who’s Winning the Peripheral Neuropathy Showdown?
Ah, diabetes! The sweet spot where too much sugar will either have you dancing with joy or, well, battling a world of medical complications that could make even a thriller movie seem dull by comparison. It’s like hosting a party where half the guests are diabetic, and only one of them has the good sense to bring a fruit salad instead of cake. Spoiler alert: 451 million folks were swinging into the diabetic disco in 2017, and that number is projected to reach a staggering 693 million by 2045! It’s all very trendy, isn’t it? And the pièce de résistance? Diabetic Peripheral Neuropathy (DPN) is the complication crashing the party – affecting about 50% of our diabetic friends!
Now, DPN isn’t just your run-of-the-mill inconvenience; it’s akin to stepping on a LEGO brick while blindfolded. It can leave you with numbness, agonizing pain, and even foot ulcers that come with an accompanying ‘you-can’t-wear-sandals’ struggle. And where does all this start? The onset is often so sneaky, many patients might think they’ve just lost sensation in their feet after a particularly long day of avoiding yoga. This neglect leads to delayed diagnoses, making early prevention and detection critically important – because the last thing you need in life is to avoid yoga and then get told that your feet are on the express train to amputation!
Let’s Get Statistical: The Science Behind the Suffering
Now, hold onto your socks because we are diving deep into some medical malarkey! DPN’s pathogenesis is a full-blown buffet of oxidative stress, inflammation, and neurotrophic dysregulation. Talk about a recipe for disaster! The infamous C-peptide, often overshadowed by its more glamorous cousin, insulin, is showing some serious promise. Studies suggest C-peptide might just have the magical touch to improve neurological function in DPN patients, but considering how complex our bodies are, ‘just’ might be the understatement of the century.
Get Your Lab Coats: Methodology Madness!
The study selected a whopping 816 patients from a hospital, making them the perfect guinea pigs to figure out the secrets of DPN and C-peptide ratio (FCP/DD, if you’re feeling formal). And just like any good reality show, there were criteria – only certain diabetics made the cut while others were left on the cutting room floor. The heroes had to be diagnosed according to WHO criteria and not have annoying complications like gestational diabetes or acute kidney drama.
Findings That’ll Make You Go “Hmm”
So, what were the results? Well, a staggering number (surprise, surprise) of patients had DPN – a full 55.76%. Age, duration of diabetes, and various comorbidities like hypertension reared their ugly heads as important factors, with the FCP/DD ratio giving them a run for their money in a battle of DPN prediction. Good news is, the FCP/DD ratio was like the quiet kid in class who turns out to be a genius – way better at predicting the likelihood of DPN than just looking at FCP or DD alone. With an AUC of 0.737, it’s got some serious smarts and leaves others in its dusty wake.
Conclusion: FCP/DD for the Win!
As we gracefully glide towards the conclusion, let’s raise our glasses (filled with low-sugar mocktails, of course) to the FCP/DD ratio! This ratio seems to express the wisdom of ancient monks combined with a mathematics PhD, turning out to be a protective factor against diabetes and its pesky friends like DPN. It’s like having an umbrella when it starts to rain – only in this case, you need it to avoid the spectacular disaster that is diabetic complications. In the sage words of a medical researcher, the FCP/DD model offers a much better predictive value than its single-rooted peers. Now, let’s give it some claps – we all could use a little applause in our lives!
Ethical Shenanigans and Funding (or lack thereof)
The study played nice and followed all ethical codes like a straight-A student, getting the thumbs-up from the Ethics Committee. And, fun fact, this research didn’t pocket any funding, making it a gladiator in the ring of medical studies. They fought valiantly—armed only with data and a passion for patient care!
Final Thoughts
So there you have it, folks! Whether you have diabetes or are simply interested in the fascinating world of peripheral neuropathy and C-peptide ratios, there’s a lot at stake in this story. It’s time to recognize that while medication is crucial, understanding these complex relationships and finding practical means for early detection can dramatically improve the quality of life significantly.
Until next time, take care of those feet, and keep those C-peptide levels in check! Otherwise, you might find yourself at the party no one wants to attend — the foot amputation event!
This article aims to keep a sharp and cheeky tone while providing the audience with important information about diabetes, DPN, and the relevance of the FCP/DD ratio in a thorough and engaging way, mimicking the observational humor of comedy legends.
How does the robust AUC of 0.737 for the FCP/DD ratio compare with traditional methods in identifying risk for diabetic peripheral neuropathy?
Ancient sage when it comes to predicting diabetic peripheral neuropathy (DPN) among patients with type 2 diabetes mellitus. With its robust AUC of 0.737, it clearly outshines traditional methods, making it a potential game-changer in clinical practice.
The FCP/DD ratio is not just another statistic; it’s a lifeline that could help healthcare professionals identify those at greater risk for DPN earlier, thereby allowing for timely interventions and better management strategies. This could translate to fewer patients experiencing the harsh consequences of DPN, such as debilitating pain and the risk of severe complications, including foot ulcers and even amputations.
The findings from this study highlight the critical importance of serum C-peptide levels and their relationship with DPN, offering hope for improved treatment protocols. By leveraging the insights gained from measuring the FCP/DD ratio, we can perhaps rewrite the narrative of diabetes management, focusing not only on glycemic control but also on preventing the neurological fallout that often accompanies the disease.
As we move forward, it’s crucial for both patients and healthcare providers to stay informed about the evolving landscape of diabetes complications. Continuous education and research are essential to combating this global epidemic, and innovative markers like the FCP/DD ratio could play a pivotal role in enhancing patient outcomes. Cheers to a future where fewer people suffer from the debilitating effects of diabetic peripheral neuropathy, thanks to smarter, evidence-based approaches to diabetes care!


