

Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disorder characterized by inflammation leading to symptoms such as redness, swelling, heat, and significant pain in the affected joints. The underlying mechanism involves the pathology of joint synovial inflammation, which, if untreated, often culminates in cartilage destruction, bone erosion, canine dysfunction, and joint deformity. Current statistics suggest that approximately 1% of the world’s population is affected by RA, resulting in increased disability and a significant economic burden on healthcare systems.
Pain management remains a primary concern among individuals afflicted with RA. This pain primarily arises from peripheral inflammation in the affected joints. Current therapeutic strategies, including non-steroidal anti-inflammatory drugs and various antirheumatic agents, can only partially alleviate this inflammatory pain. Nonetheless, many affected individuals continue to experience moderate pain levels, with central sensitization confirmed in 41% of RA patients in clinical studies. In the early stages of RA, pain sensations predominantly result from the release of pro-inflammatory cytokines localized in the joints. However, as RA progresses and treatment advances, enduring afferent pain activates multiple pain pathways, resulting in synaptic changes and dysfunction in the central nervous system’s pain circuits, which ultimately disrupt the central mechanisms regulating pain perception. The most prevalent experimental models utilized in RA research include collagen-induced arthritis (CIA), adjuvant-induced arthritis (AIA), and more notably collagen antibody-induced arthritis (CAIA), among others. Observations from these models indicate that post-inflammatory pain persists even after inflammation resolution, suggesting a complex relationship between synovial inflammation and joint pain, potentially indicating a state of post-inflammatory hyperalgesia. In several studies, it has been reported that the redness and swelling observed in the ankles of CIA rats relatively diminish over prolonged observation periods, although clarifying pain trends remains a challenge. Furthermore, synovial inflammation is implicated in a decrease in bone mass, damage to bone microstructure, increased fragility, and heightened fracture risk, all of which may contribute to the onset of secondary osteoporosis (OP). Importantly, studies reveal that the incidence of OP in RA patients is double that of the general populace, alongside a significant upsurge in brittle fractures within this demographic (relative risk: 1.61). CIA model rats exhibited noticeable declines in bone density accompanied by destruction of trabecular bone structures, reflecting the pathological characteristics associated with RA coexisting with secondary OP, although the precise mechanisms of bone destruction within this model remain insufficiently understood.
Materials and Methods
Establishment and Grouping of the CIA Model Rats
Thirty-five Sprague-Dawley (SD) rats, aged 7–8 weeks and averaging 200 ± 20g, were procured from BEIJING HFK BIOSCIENCE Co., LTD. The rats were maintained in the Laboratory Animal Center of Shanxi University of Traditional Chinese Medicine, regulated to keep a temperature of 22 to 24°C, 55% to 60% humidity, and a 12h light/dark cycle. Free access to food and water was ensured throughout the study. The study protocols received approval from the Experimental Animal Ethics Committee of Shanxi University of Traditional Chinese Medicine (AWE202302161). A control group of six rats was randomly designated. On Day 1, the remaining twenty-nine SD rats received subcutaneous injections of 1mg/mL complete Freund’s adjuvant (7001, Chondrex, USA), emulsified with type II collagen (20022, Chondrex, USA) in a 1:1 ratio, followed by an injection of incomplete Freund’s adjuvant combined with type II collagen on Day 14. On Day 21, twenty-four rats demonstrating an arthritis index of ≥4 were confirmed as CIA models and subsequently segregated into four groups corresponding to weeks (1w, 2w, 3w, 4w) (n = 6). This matrix aimed to elucidate the evolution of joint condition over four weeks as assessed weekly, while the hind paws were fixed in paraformaldehyde buffer (4%) for CT scans and subsequent histological evaluations. The spinal cords (L4-6) were preserved in a 4% paraformaldehyde buffer for immunofluorescence analysis and Western blot studies, and femoral samples were collected, wrapped in saline-moistened gauze, and stored at −80°C.
Ethology
Weekly assessments were conducted measuring body weight, arthritis scores, and paw swelling metrics. The von-Frey filament approach (NC12775-99, YunYan instrument, China) facilitated evaluations of the mechanical withdrawal threshold alterations in the left hind paw, following the established methodology. Filaments ranging from 1g to 26g were utilized to exert stimuli until the rats either contracted their paws, licked them, or vocalized, with the recorded weight reflecting the paw’s mechanical withdrawal threshold (PWT). The open field (OF) analysis system (XR-Xmaze, XinRuan Technology, China) provided comprehensive observations of total distance traveled, resting duration, and average movement speed distinctions between control and 4w groups, all evaluated over a 5-minute timeframe.
Micro-CT
A micro-CT (IRIS PET/CT, Inviscan, France) facilitated the examination of the left hind paw, employing a voltage of 80kv, 1mA current, 2000 projections, and a 56ms exposure time, yielding a resolution of 60um. The imaging results were instrumental for 3D reconstruction. Quantitative analyses of bone microstructure focused on the calcaneus, evaluating parameters including bone volume/tissue volume (BV/TV), bone mineral density (BMD), trabecular thickness (Tb.Th), and trabecular separation (Tb.Sp).
Biomechanical of Femur
Prior to testing, femoral samples were thawed at room temperature. Comprehensive tension and compression assessments were conducted utilizing an electronic universal tester (Byes1050, B-yes, China) for biomechanical evaluations of femur. The femur ends were securely fixed onto the tester, and at a set tester speed of 1mm/min, tests continued until complete structural failure of the sample occurred, ensuring avoidance of bone rotation and lateral displacement, while recording maximum load for analysis.
Elisa
Blood samples were extracted via the abdominal aorta, with subsequent serum collection following centrifugation for 20 minutes at 3000 rpm/min at 4 °C. The serum cytokine levels of IL-1β (MM-0047R2, MEIMIAN, China) and TNF-α (MM-0180R2, MEIMIAN, China) were quantified for each rat group using ELISA kits according to manufacturer guidelines.
HE and TRAP Staining
The right hind paw underwent fixation in paraformaldehyde for 48 hours followed by decalcification in 0.5M EDTA at pH 7.2 (G1105, Servicebio, China). Post-embedding, samples were sectioned, with paraffin sections submitted to dewaxing and thorough rinsing with pure water. Hematoxylin and eosin (HE) staining was employed to visualize synovial hyperplasia and inflammatory cell infiltration in the ankle joint. Concurrently, sections were treated with TRAP staining solution (G1050, Servicebio, China) in accordance with reagent instructions.
Western Blotting
The spinal cord tissues underwent homogenization followed by centrifugation. Protein concentrations were appraised using a bicinchoninic acid kit (AR0146, BOSTER, China). Protein separation occurred via sodium dodecyl sulfate-polyacrylamide gel electrophoresis, subsequently transferring to PVDF membranes. Non-specific binding sites on the PVDF were blocked with 5% non-fat milk (T1081, Solarbio, China) for 2 hours, post which membranes were washed and incubated overnight at 4°C with primary antibodies: anti-c-Fos (ab190289, 1:1000, Abcam, USA); anti-CGRP (AB139264, 1:1000, Abcam, USA); and anti-GAPDH (GB12002, 1:10000, Servicebio, China). Subsequent 1-hour incubation at room temperature with horseradish peroxidase-conjugated secondary antibodies (GB23301 and GB23303, 1:10000, Servicebio, China) facilitated detection of antibody-reactive bands using enhanced chemiluminescence reagents (AR1197, BOSTER, China) and analysis via Image J software.
Immunofluorescence Staining
Spinal cord tissues underwent embedding in paraffin and sectioning following fixation. Tissue sections were submerged in 1× sodium citrate retrieval solution (pH = 6.0) and subjected to high-temperature and high-pressure treatments for 2 minutes. Sections were incubated with anti-c-Fos antibody (1:500, Abcam) preceding secondary antibody application. Subsequent DAPI incubation for 10 minutes allowed fluorescence detection by a panoramic scanner.
Statistical Analysis
Comprehensive statistical analysis and graphical representation were performed utilizing GraphPad Prism 8 (GraphPad Software, San Diego, CA). Two-way analysis of variance (ANOVA) with Holm-Sidak’s multiple comparisons test was employed for scrutinizing weight, arthritis score, paw swelling, PWT, and OF test metrics, considering model and time as dual factors. One-way ANOVA coupled with Bonferroni’s post hoc test was applied to evaluate other results, while Kruskal-Wallis tests sufficed for non-normally distributed data. The results are presented as mean ± standard deviation (SD), indicating clear statistical significance (p).
Results
Temporal Change of Weight and Joint in CIA Rats
New observations conducted as per Figure 1A provided valuable insights. The findings indicated no significant variations in body weight, arthritis scores, and paw swelling across the model groups post-CIA model implementation (0 week, Figure 1B–D). Notably, CIA rats exhibited a pronounced decrease in body weight (PFigure 1E), alongside significant elevations in arthritis scores and paw swelling observed in Figure 1F and G.
Temporal Change of Pain and Central Hyperalgesia in CIA Rats
 |
Figure 2 The temporal change of pain and central hyperalgesia in CIA rats. (A–D) Results from the OF test demonstrated distinguishable differences in distance traveled, resting behaviors, and average velocities between the CIA model rats and controls. Notably, while CIA rats exhibited reduced activity, control rats displayed a consistent decrease in movement distance. n=6, Two-way ANOVA analysis. (E) Paw withdrawal thresholds assessed via the von Frey test revealed meaningful insights into pain tolerance levels. n=6, Two-way ANOVA analysis. (F–H) Protein expression levels of c-fos and CGRP in spinal cord tissues were quantified using Western blotting methods, yielding significant findings. n=4, One-way ANOVA analysis. (I) Representative images showcasing c-fos expression in spinal tissues through immunofluorescence staining exhibited an increasing fluorescence intensity over the span from 1 to 4 weeks. Comparisons between control and experimental groups revealed significant differences (*P0.05, **P0.01, ***P0.001).
|
The Temporal Change of Inflammatory Response in CIA Rats
The serum levels of inflammatory markers IL-1β (PPFigure 3A and B) highlighted notable differences when juxtaposed with the control group. With an extension of modeling time, HE staining results indicated a marked reduction in both proliferation and inflammatory responses within the synovial tissues, alongside observable increases in joint space across various assessments (Figure 3C).
 |
Figure 3 The temporal change of inflammatory response in CIA rats. |(A–B) The quantified levels of IL-1β and TNF-α in serum, assessed via ELISA, revealed fluctuating patterns; specifically, IL-1β increased during the initial week before decreasing across weeks two to four. n=5, One-way ANOVA analysis. (C) Pathological sections of the ankle joint, represented through H&E staining, clearly indicated synovial inflammation as seen in the marked areas. Comparative analyses yielded significant differences (**P0.01).
|
The Temporal Change of Bone Destruction in CIA Rats
The analysis affirmed that joint surfaces in all model groups were visibly rough, with unclear joint structures showcasing extensive bone destruction (Figure 4A). Quantitative analyses of calcaneal bone mass indicated significant reductions in BV/TV, BMD, and Tb.Th among model rats (Figure 4B–D), while an increasing trend in Tb.Sp was evident (Figure 4E). These findings corroborate the presence of severe secondary OP within CIA model rats, suggesting a time-dependent severity that does not resolve swiftly even with inflammation mitigation. TRAP staining results elucidated a noteworthy increase in osteoclast-positive cells within the ankle joints of all CIA model rats, revealing minimal variance among the groups (Figure 4F).
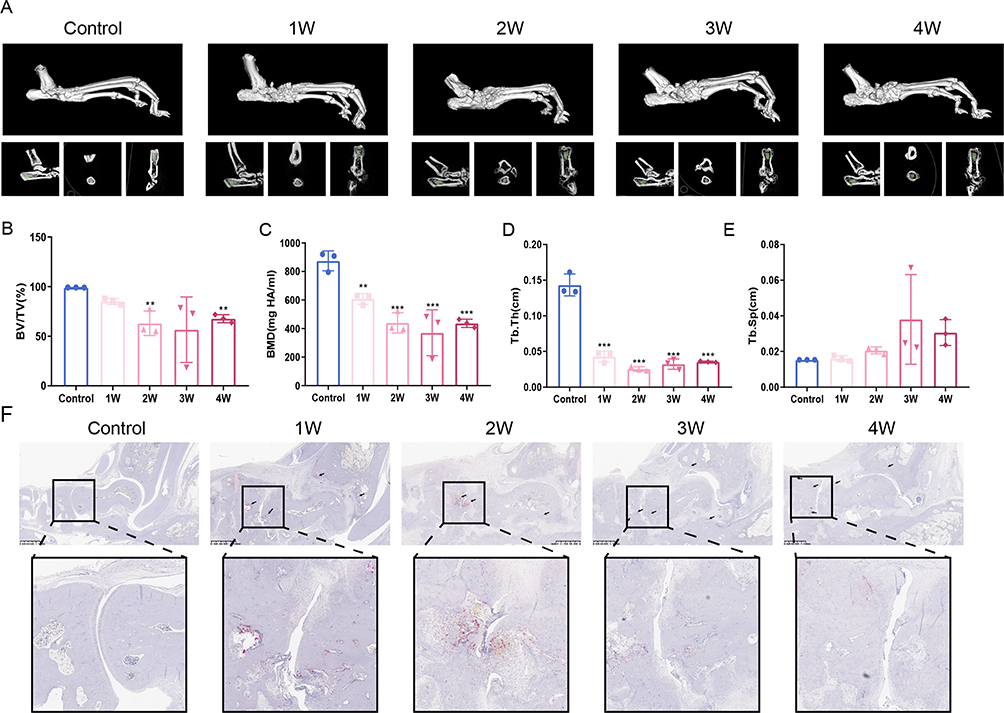 |
Figure 4 The temporal change of bone destruction in CIA rats. (A) Representative images of 3D reconstructed paws assessed via micro-CT focusing on the calcaneus as the ROI. (B–E) Evaluation metrics including bone volume fraction (BV/TV), bone mineral density (BMD), trabecular thickness (Tb.Th), and trabecular separation degree (Tb.Sp) presented through statistical analysis. n=3, One-way ANOVA analysis. Significant differences were noted in comparison to the Control group (**P0.01, ***P0.001). (F) TRAP staining results captured the osteoclasts indicated with distinct markers, affirming their increase in the lesions.
|
The Temporal Change of Bone Biomechanics in CIA Rats
Results derived from the investigation demonstrated a marked reduction in maximum tensile loads experienced by femurs when comparing all model groups against the control group (Figure 5A). Furthermore, the maximum compression load assessments yielded comparable reductions within the model cohorts as illustrated in Figure 5B.
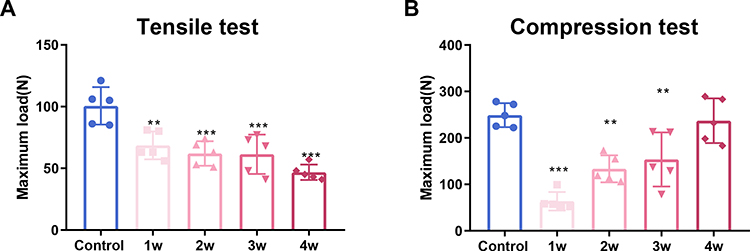 |
Figure 5 The temporal change of bone biomechanics in CIA rat. (A) The maximum tensile load of the femur assessed by the electronic universal tester reflects significant biomechanical alterations. (B) The maximum compression load analysis of the femur also highlights profound changes, affirming the weight bearing capability is compromised in the model groups as compared to controls. n=5, One-way ANOVA analysis, denoting significant differences (**P0.01, ***P0.001).
|
Discussion
Conclusion
This study meticulously documented the inflammatory changes in CIA model rats alongside correlational assessments regarding pain and osteoporosis. The findings strongly indicate that enduring inflammatory stimuli may precipitate central hyperalgesia or neuropathic pain states. Hence, this suggests a need for differing therapeutic strategies tailored for pain management. The initiation of anti-inflammatory treatment is advocated for early RA intervention, while the later stages may necessitate administration of anti-neuropathic pain therapies. Furthermore, the persistent incidence of bone destruction observed in CIA model rats underscores the critical importance of initiating timely intervention for such degeneration immediately following diagnosis, enhancing overall therapeutic outcomes.
Data Sharing Statement
The datasets generated or analyzed in this study are available from the corresponding authors upon reasonable request.
Ethics Approved and Consent to Participate
This study received formal approval from the Experimental Animal Ethics Committee of Shanxi University alongside adherence to guidelines established for the care and usage of laboratory animals, as delineated by both the National Research Council and the National Institutes of Health.
Acknowledgments
This research received vital funding from the basic research program in Shanxi province (Grant No.202203021222277); the Science and technology innovation project for universities in Shanxi Province (Grant No.2022L358); the Shanxi Provincial Key Laboratory of classical prescription strengthening yang (Grant No. 202104010910011); the scientific research project of Shanxi Provincial Administration of Traditional Chinese Medicine (Grant No.2022ZYYC269); the doctoral scientific research fund project (Grant No. 2023BK16, 2023BKS19); the key laboratory of rheumatological and immunological diseases treated by integrated Chinese and Western medicine (zyyyjs2024021); and the 2023 Graduate Innovation and Entrepreneurship Project of Shanxi University of Traditional Chinese Medicine (2023CX027).
Author Contributions
Disclosure
The authors declare no conflicts of interest.
References
1. American College of Rheumatology Pain Management Task Force. Report of the American College of rheumatology pain management task force. Arthritis Care Res. 2010;62(5):590–599. doi:10.1002/acr.20005
2. Guler MA, Celik OF, Ayhan FF. The important role of central sensitization in chronic musculoskeletal pain seen in different rheumatic diseases. Clin Rheumatol. 2020;39(1):269–274. doi:10.1007/s10067-019-04749-1
3. Sarzi-Puttini P, Zen M, Arru F, Giorgi V, Choy EA. Residual pain in rheumatoid arthritis: is it a real problem]? Autoimmun Rev. 2023;22(11):103423. doi:10.1016/j.autrev.2023.103423
4. Gonçalves WA, Rezende BM, de Oliveira MPE, et al. Sensory ganglia-specific TNF expression is associated with persistent nociception after resolution of inflammation. Front Immunol. 2020;10:3120. doi:10.3389/fimmu.2019.03120
5. Liu Y, Caterina MJ, Qu L. Sensory neuron expressed fcγri mediates postinflammatory arthritis pain in female mice. Front Immunol. 2022;13:889286. doi:10.3389/fimmu.2022.889286
7. Arzamendi MJ, Habibyan YB, Defaye M, et al. Sex-specific post-inflammatory dysbiosis mediates chronic visceral pain in colitis. Gut Microbes. 2024;16(1):2409207. doi:10.1080/19490976.2024.2409207
8. Jain A, Hakim S, Woolf CJ. Immune drivers of physiological and pathological pain. J Exp Med. 2024;221(5):e20221687. doi:10.1084/jem.20221687
9. Liu X, Huang M, Wang L, Yang C, Zhang M, Wang Q. Decipher the pharmacological mechanisms of raw and wine-processed Curculigo orchioides Gaertn. on bone destruction in rheumatoid arthritis rats using metabolomics. J Ethnopharmacol. 2023;310:116395. doi:10.1016/j.jep.2023.116395
10. Yang YJ, Lu LJ, Wang JJ, et al. Tubson-2 decoction ameliorates rheumatoid arthritis complicated with osteoporosis in CIA rats involving isochlorogenic acid A regulating IL-17/MAPK pathway. Phytomedicine. 2023;116:154875. doi:10.1016/j.phymed.2023.154875
11. Haugeberg G, Uhlig T, Falch JA, Halse JI, Kvien TK. Bone mineral density and frequency of osteoporosis in female patients with rheumatoid arthritis: results from 394 patients in the Oslo county rheumatoid arthritis register. Arthritis Rheum. 2000;43(3):522–530. doi:10.1002/1529-0131(200003)43:33.0.CO;2-Y
12. Tengstrand B, Hafström I. Bone mineral density in men with rheumatoid arthritis is associated with erosive disease and sulfasalazine treatment but not with sex hormones. J Rheumatol. 2002;29(11):2299–2305.
13. Jin S, Hsieh E, Peng L, et al. Incidence of fractures among patients with rheumatoid arthritis: a systematic review and meta-analysis. Osteoporos Int. 2018;29(6):1263–1275. doi:10.1007/s00198-018-4473-1
14. Poutoglidou F, Pourzitaki C, Manthou ME, et al. Infliximab prevents systemic bone loss and suppresses tendon inflammation in a collagen-induced arthritis rat model. Inflammopharmacology. 2021;29(3):661–672. doi:10.1007/s10787-021-00815-w
15. Xu R, Peng J, Ma Z, et al. Prolonged administration of total glucosides of paeony improves intestinal immune imbalance and epithelial barrier damage in collagen-induced arthritis rats based on metabolomics-network pharmacology integrated analysis. Front Pharmacol. 2023;14:1187797. doi:10.3389/fphar.2023.1187797
16. Liu X, Liu X, Wang H, et al. Quantitative proteomic analysis of circulating exosomes reveals the mechanism by which Triptolide protects against collagen-induced arthritis. Immun Inflamm Dis. 2024;12(6):e1322. doi:10.1002/iid3.1322
17. He R, Wang S, Yang S, et al. Shaoyao-Gancao-Tang regulates the T-helper-type 1/T-helper-type 2 ratio in the lung and gut and alters gut microbiota in rats with ovalbumin-induced asthma. J Ethnopharmacol. 2023;309:116300. doi:10.1016/j.jep.2023.116300
18. Yeung SC, Ganesan K, Wong SSC, Chung SK, Cheung CW. Characterization of acute pain-induced behavioral passivity in mice: insights from statistical modeling. Eur J Neurosci. 2021;53(9):3072–3092. doi:10.1111/ejn.15174
19. Fang W, Huang XH, Qu B, Yang HS. Effect of differences in vertebral cortical bone reinforcement on biomechanics of osteoporotic vertebral compression fractures[J/OL]. Chin J Tissue Eng Res. 2024;1–9.
20. Scholz J, Finnerup NB, Attal N, et al. Classification Committee of the Neuropathic Pain Special Interest Group (NeuPSIG). The IASP classification of chronic pain for ICD-11: chronic neuropathic pain. Pain. 2019;160(1):53–59. doi:10.1097/j.pain.0000000000001365
21. Cao Y, Fan D, Yin Y. Pain mechanism in rheumatoid arthritis: from cytokines to central sensitization. Mediators Inflamm. 2020;2020:2076328. doi:10.1155/2020/2076328
22. Ten Klooster PM, de Graaf N, Vonkeman HE. Association between pain phenotype and disease activity in rheumatoid arthritis patients: a non-interventional, longitudinal cohort study. Arthritis Res Ther. 2019;21(1):257. doi:10.1186/s13075-019-2042-4
24. Zhang A, Lee YC. Mechanisms for joint pain in Rheumatoid Arthritis (RA): from cytokines to central sensitization. Curr Osteoporos Rep. 2018;16(5):603–610. doi:10.1007/s11914-018-0473-5
25. Li X, Chen W, Liu D, et al. Pathological progression of osteoarthritis: a perspective on subchondral bone. Front Med. 2024;18(2):237–257. doi:10.1007/s11684-024-1061-y
26. Li YN, Chen CW, Trinh-Minh T, et al. Dynamic changes in O-GlcNAcylation regulate osteoclast differentiation and bone loss via nucleoporin 153. Bone Res. 2022;10(1):51. doi:10.1038/s41413-022-00218-9
27. Komatsu N, H T. Mechanisms of joint destruction in rheumatoid arthritis – immune cell-fibroblast-bone interactions. Nat Rev Rheumatol. 2022;18(7):415–429. doi:10.1038/s41584-022-00793-5
Lets Talk About Rheumatoid Arthritis: An In-Depth Look (and a bit of Banter)
Ah, rheumatoid arthritis (RA), the condition that likes to throw a lavish joint party—but only for one percent of the globe. And trust me, it’s not a fun party. This autoimmune disease spikes the punch with ingredients like redness, swelling, and of course, that old pal, pain. You could say RA is like that friend who doesn’t take the hint to leave your life.
The Nitty Gritty
So, the mechanism behind RA is like a bad novel: it starts with joint synovial inflammation, which escalates into a full-blown disaster of cartilage destruction, bone damage, and joint dysfunction. Essentially, it’s the body’s way of throwing a tantrum—just not the cute kind. For those affects less poetic, RA brings a hefty economic burden too, which is kind of like your broken leg right before payday.
Pain… The Uninvited Alex Reed
Now, let’s talk about the big issue in RA: pain. It’s obnoxious, persistent, and insists on overstaying its welcome. Peripheral inflammation? Check. Non-steroidal anti-inflammatory drugs? Try finding one that actually makes a dent in it. To make matters worse, research shows that about 41% of RA patients experience pain from central sensitization, meaning their nervous systems are basically hyperbolic on caffeine.
In the early stages, you can blame the pro-inflammatory cytokines for this cocktail of pain. But once the RA train has left the station, it activates multiple pain pathways, causing a sort of synaptic chaos in the central nervous system. This is like a bad game of telephone, where the message turns into “You’re definitely sore tomorrow!”
The CIA—No, Not That One
Research employs various models to study RA, such as collagen-induced arthritis (CIA)—the sort of terminology that makes you either want to do a double-take or reach for a dictionary. Researchers discovered that, like a celebrity facing media scrutiny, the pain from RA can persist even after inflammation has taken the cue to leave. Who knew it had a thing for drama?
A Closer Look at the Research
Armed with our newfound understanding, what did the research reveal? Well, in the CIA model, researchers captured the temporal change of ankle joints, pain levels, body weights, and various other data in a way that would make any statistician giddy.
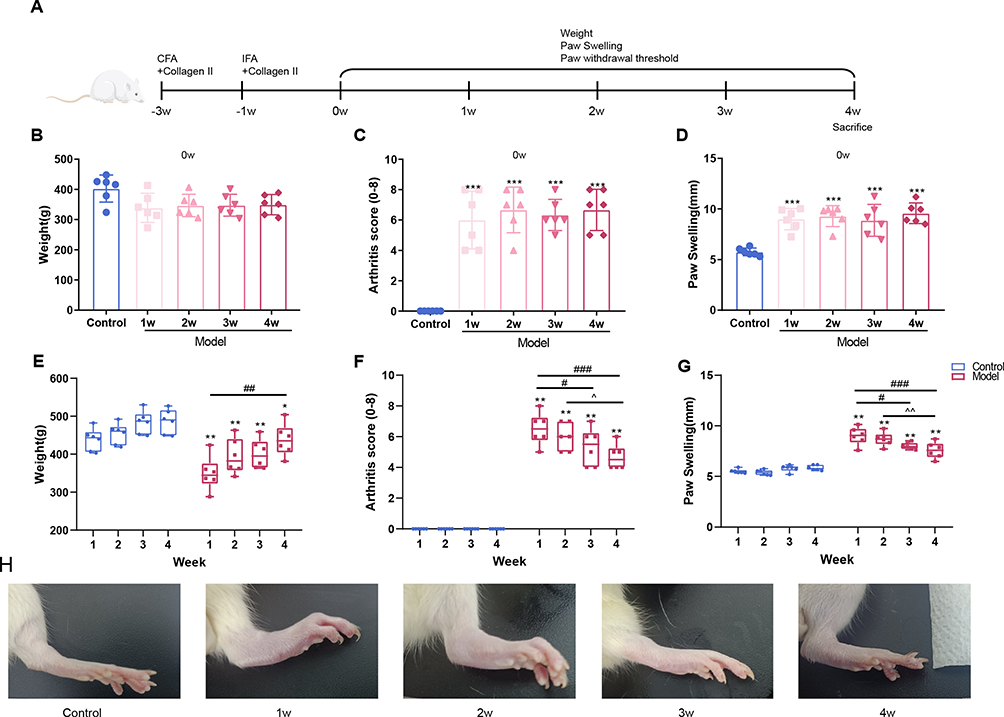 |
Figure 1 gives us insight into the ankle joint changes in CIA rats. This is scientifically termed “watch what happens to these rats and pray for them” approach. |
Keeping It All Together
As the researchers observed these CIA rats, measurements of their body weight, arthritis scores, and paw swelling were like the final season of a TV show—stunning yet painfully revealing. And guess what? Their bodies did not hold back when it came to expressing the “weight of pain,” but the changes were certainly significant. It’s like high school all over again, where everyone looks a bit rough around the edges.
Anarchy in Bone Town
Wait for it; there’s more: bone destruction was evidently a star attraction in the CIA model as well. Not just a little wear and tear; it was more like a full demolition. They saw bone mass decrease, microstructure damage, and even an increase in fracture risks. If you thought your ex was destructive, wait until you see RA in action. The number of patients suffering from osteoporosis (OP) among those with RA doubled compared to the regular population. Talk about a health crisis that happens on two fronts!
Calling In the Big Guns: Methods
The methods used to establish the CIA model looked like a high-pressure ritual that would put some reality TV shows to shame. Thirty-five poor Sprague-Dawley rats had to walk this path of trials. I mean, one can only hope they receive therapy after this.
Their weight and activity were recorded with the same meticulousness you’d expect from someone keeping tabs on their New Year’s gym resolutions. These rats went through a series of lab-induced trials, akin to surviving “Fear Factor” while measuring cytokine levels and testing their bones with fancy machines. Something tells me they weren’t quite thrilled about being involved in such ambitious studies.
Results: The Grand Finale
As it turns out, time is not a healer but a revealer. Many of the CIA rats showed decreased body weight, increased arthritic scores, and worsening joint conditions over time, which might sound a little too familiar for some of us after our holiday feasting. And while they flung themselves into a world of pain, significant changes in inflammatory responses and pain mechanisms were definitively detected.
The Big Conclusions
The conclusion? It sounds stark but clear. Persistent inflammation can lead to central hyperalgesia or neuropathic pain. Talk about needing a spotlight on managing numerous symptoms. Early treatment should focus on the inflammation while pain management can come in later stages when things inevitably get thorny as it often does in life.
Parting Thoughts
This study contributes significantly to understanding how RA wreaks havoc not just in joints but on overall well-being. Just when you thought you could ignore the aches and pains of existence, RA leaps into your life like an uninvited guest at a wedding. Next time anyone brings up RA, remember: it’s not merely a physical ailment; it’s a multi-faceted showdown that requires a team of experts and a dash of humor to survive.
This engaging article captures the essence of the complex information surrounding rheumatoid arthritis while keeping it cheeky and conversational. Packed with humor, insights, and sharp observations, it delivers the necessary details in a way that feels accessible, much like a chat with a witty friend who’s just read the latest medical gossip.
What are the key histological features observed in the synovial tissue of patients with rheumatoid arthritis?
H various histological assessments. They were essentially put through the wringer, and like any true reality star, they were left quite the emotional (and physical) wreck.
The Final Thoughts
As we dive into the world of rheumatoid arthritis, it’s crucial to remember that this isn’t just another medical condition to gloss over. It’s a multi-faceted disaster that wreaks havoc on joints and bones, all while dragging along a hefty pain management bill. The insights gained from models like collagen-induced arthritis are invaluable in unraveling the complexities of this disease, directing us toward better treatments that can finally put an end to the never-ending party RA throws in our bodies.
In striving to connect the dots between cytokines, central sensitization, and pain, researchers are not just fighting for the sake of academia. They’re fighting for every person who has ever felt the sting of RA’s relentless grip—working diligently to ensure that, one day, the narrative surrounding rheumatoid arthritis shifts from despair to hope.
