
{kind=link}
2024-04-01 03:03:57
He Colorectal cancer It has a high prevalence worldwide. Efforts are increasingly being added for its early detection and treatment. In this sense, Chung and collaborators from Harvard Medical School (Boston, USA) used a non-invasive assay of Free DNA (ctDNA) in plasma to detect the pathology in an average risk population in the United States.
Free DNA is found in body fluids, such as plasma and urine. It can be analyzed by using methods that are sensitive enough to detect low concentrations, such as PCR assay and sequencing. The DNA methylation is the most common epigenetic signature analyzed. To know the methylation status of a fragment, it can be treated with a reagent that cleaves or binds to it, depending on whether it is methylated or not. This was the approach used by Chung’s team. A more recent development is the direct detection of methylation by single molecule sequencing del ADNct.
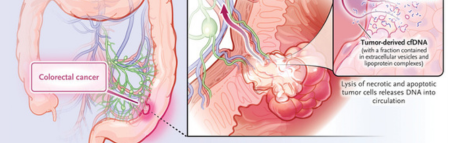
Tumor-derived DNA can be found in plasma free DNA obtained from cancer patients, a finding that supports the experimental use of this molecule for the detection, monitoring and prognosis of the pathology.
The research led by Chung used a commercially available assay to analyze ctDNA in the plasma of 7,861 people with an average age of 60 years. The test characterizes and then integrates three types of information regarding the person’s ctDNA: methylation status, aberrant fragmentation patterns, and the presence or absence of somatic pathogenic variants in the genes APC y KRAS (Figure 1). Using this test, the sensitivity of detecting colorectal cancer was 83%, of which advanced neoplasia 90% and advanced precancerous lesions (including adenomatous polyps advanced and sessile serrated lesions) of 13%. Specificity for the detection of advanced neoplasia was inversely correlated with age.
Figure 1: Detection of colorectal cancer with the use of free DNA (ctDNA).
Although in this work they demonstrated the feasibility of using plasma ctDNA to detect the disease, the relatively low sensitivity in the case of advanced precancerous lesions is a limitation. Furthermore, colonoscopy not only detects these lesions with high sensitivity, but also allows their immediate removal. However, the non-invasive nature of the plasma ctDNA assay is a feature that is likely to result in greater acceptance than the colonoscopy, for which it is necessary to evaluate the cost-benefit and thus justify its implementation. Fecal tests are also an option, as reported by other studies.
Although the Chung et al. trial used different ctDNA information, the relative contributions of each of these components to the final result are weak and may vary between patients and populations. The possibility of decreased test specificity with age, thought to be related to DNA methylation, also requires further investigation. The fact that false positives can arise in people with non-colorectal cancers represents another line of study. Indeed, aberrant ctDNA methylation and fragmentation profiles have been reported for multiple tumor types.
According to the authors of the work, the test manufacturer recommends an interval of 3 years between this type of molecular tests. A study of plasma ctDNA for the detection of nasopharyngeal carcinoma showed that people with a positive test, but without an immediately identifiable neoplasm, had a higher risk of the pathology in the future. If a similar phenomenon occurs in people at risk for colorectal cancer, perhaps the interval for repeat ctDNA screening or in turn the scheduling of conventional invasive screening might be adapted according to the results of previous ctDNA testing.
Bibliographic source
Cell-free DNA for Colorectal Cancer Screening
Y.M. Dennis Lo, B.M., B.Ch., D.Phil., D.M.
State Key Laboratory of Translational Oncology, Department of Chemical Pathology
N Engl J Med 2024; 390:1047-1050
1711941278
#SAVALnet #Science #Medicine